

Dermoscopy in female androgenic alopecia: method standardization and diagnostic criteria
- PMID: 20927234
- PMCID: PMC2938574
- DOI: 10.4103/0974-7753.58555
Dermoscopy in female androgenic alopecia: method standardization and diagnostic criteria
Abstract
Objective: Establishing the trichoscopy criteria of female androgenic alopecia (FAGA).
Design: Trichoscopy images were retrospectively evaluated.
Setting: Dermatologic hospital-based clinic and private practice offices.
Patients and methods: One hundred and thirty-one females (59 with androgenic alopecia, 33 with chronic telogen effluvium (CTE), 39 healthy controls). The diagnosis was based on clinical examination and confirmed by histopatology.
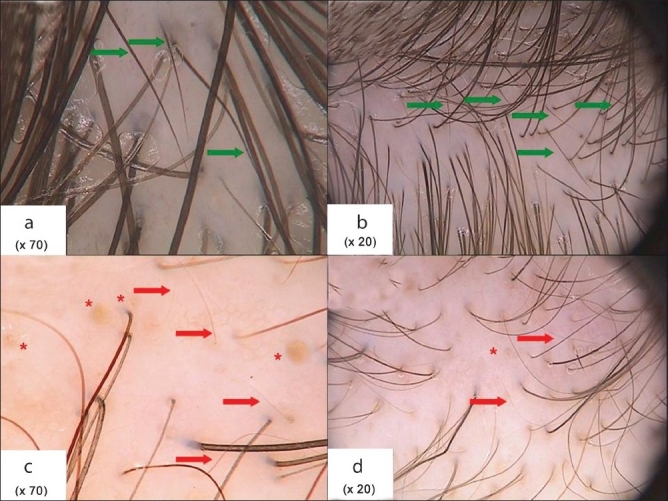
Main outcome measure: Trichoscopy results obtained in frontal, occipital and both temporal areas of the scalp under a 20-fold and 70-fold magnification, including average hair thickness, number of 'yellow dots' and vellus hairs, number of hairs in one pilosebaceous unit and percentage of follicular ostia with perifollicullar hyperpigmentation.
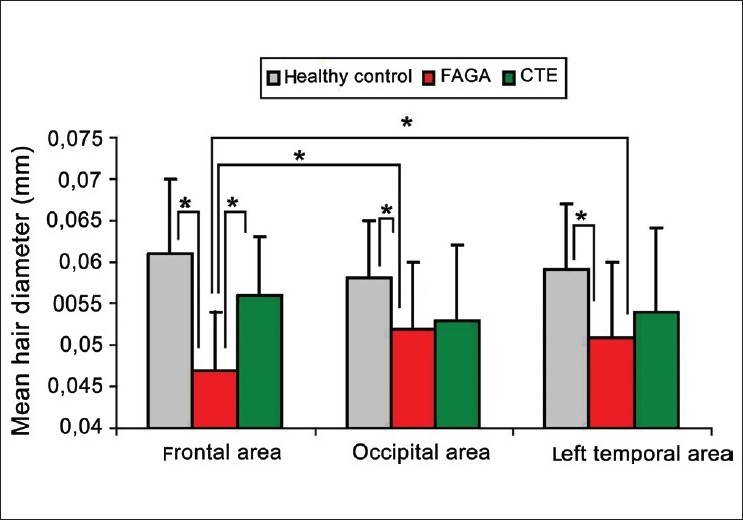
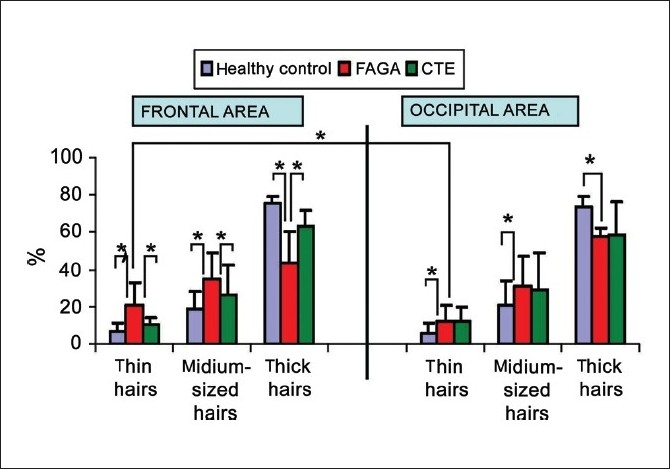
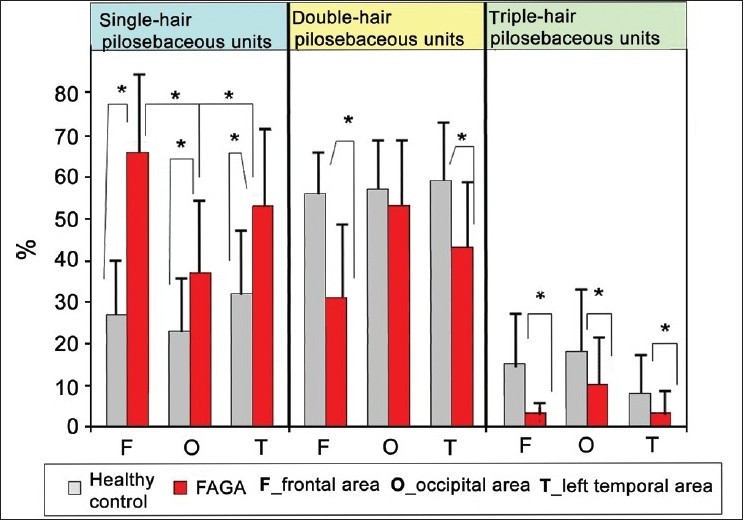
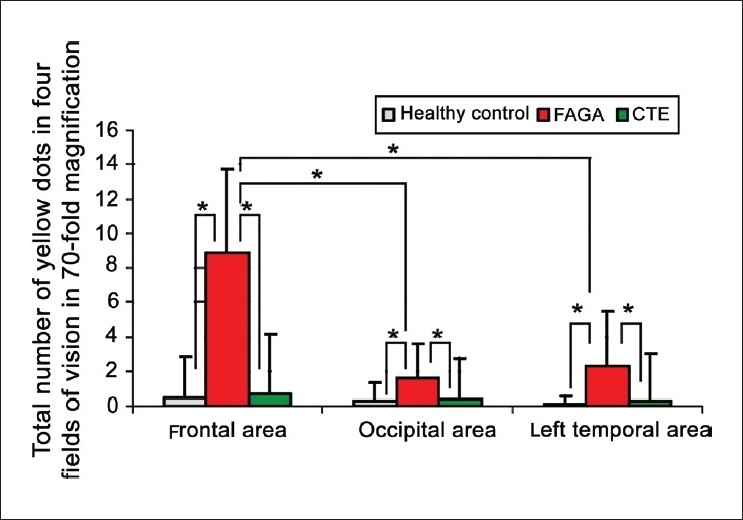
Results: Average hair thickness in frontal area versus occiput was, respectively, 0.061 ± 0.008 mm versus 0.058 ± 0.007 mm in healthy controls, 0.047 ± 0.007 mm versus 0.052 ± 0.008 mm in androgenic alopecia and 0.056 ± 0.007 mm versus 0.053 ± 0.009 mm in CTE. Mean percentage of thin hairs (< 0.03 mm) in androgenic alopecia was 20.9 ± 12% and was significantly higher than in healthy controls (6.15 ± 4.6%, P < 0.001) or in CTE (10.4 ± 3.9%, P < 0.001). The number of yellow dots, pilosebaceous units with only one hair and with perifollicular hyperpigmentation was significantly increased in androgenic alopecia. Classification and Regression Tree Analysis was performed to establish diagnostic criteria for FAGA.
Conclusion: FAGA may be differentiated from CTE based on trichoscopy criteria. Major criteria are ratio of (1) more than four yellow dots in four images (70-fold magnification) in the frontal area, (2) lower average hair thickness in the frontal area compared to the occiput and (3) more than 10% of thin hairs (below 0.03 mm) in the frontal area. Minor criteria encompass increased frontal to occipital ratio of (1) single-hair pilosebaceous units, (2) vellus hairs and (3) perifollicular discoloration. Fulfillment of two major criteria or one major and two minor criteria allows to diagnose FAGA based on trichoscopy with a 98% specificity.
Keywords: Alopecia; dermoscopy; hair; trichoscopy; videodermoscopy.
Conflict of interest statement
Figures
References
-
- van Neste D. Female patients complaining about hair loss: Documentation of defective scalp hair dynamics with contrast-enhanced phototrichogram. Skin Res Technol. 2006;12:83–8. - PubMed
-
- Sinclair R, Jolley D, Mallari R, Magee J. The reliability of horizontally sectioned scalp biopses in the diagnosis of chronic diffuse telogen hair loss in women. J Am Acad Dermatol. 2004;51:189–99. - PubMed
-
- Whiting D. Chronic telogen effluvium. Dermatol Clin. 1996;14:697–11. - PubMed
-
- Harrison S, Sinclair R. Telogen effluvium. Clin Exp Dermatol. 2003;27:389–5. - PubMed
-
- Sinclair R. Chronic telogen effluvium or early androgenic alopecia? Int J Dermatol. 2004;43:842–3. - PubMed
LinkOut - more resources
Full Text Sources
Medical
