

Hypertrophic scarring and keloids: pathomechanisms and current and emerging treatment strategies
- PMID: 20927486
- PMCID: PMC3022978
- DOI: 10.2119/molmed.2009.00153
Hypertrophic scarring and keloids: pathomechanisms and current and emerging treatment strategies
Abstract
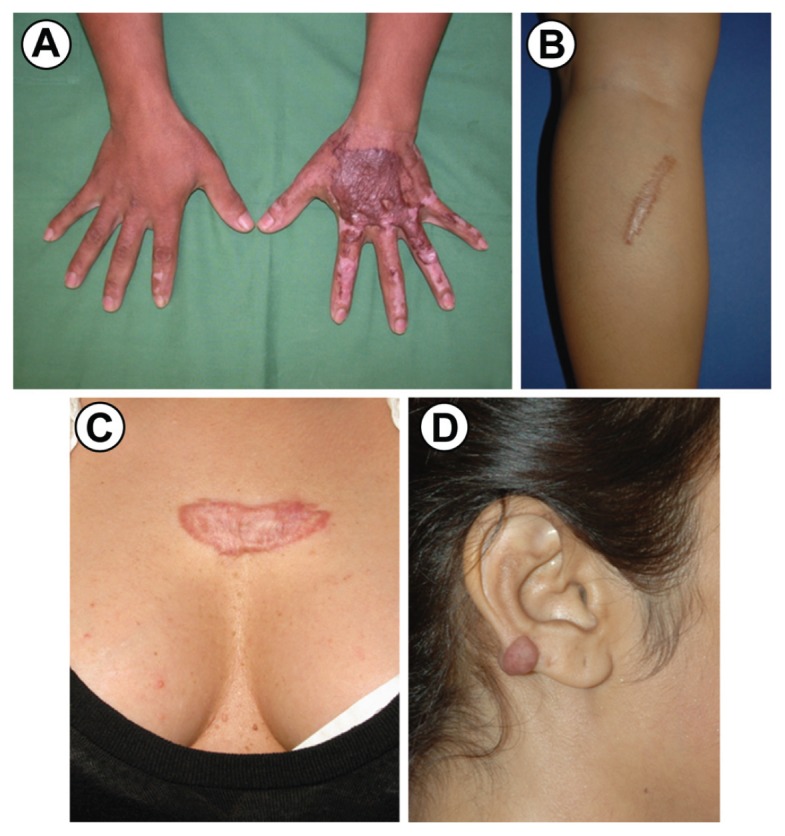
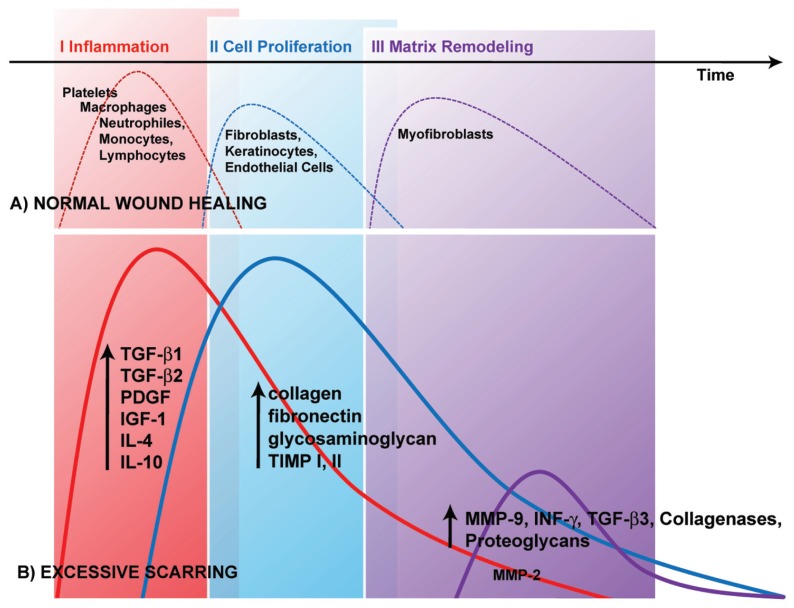
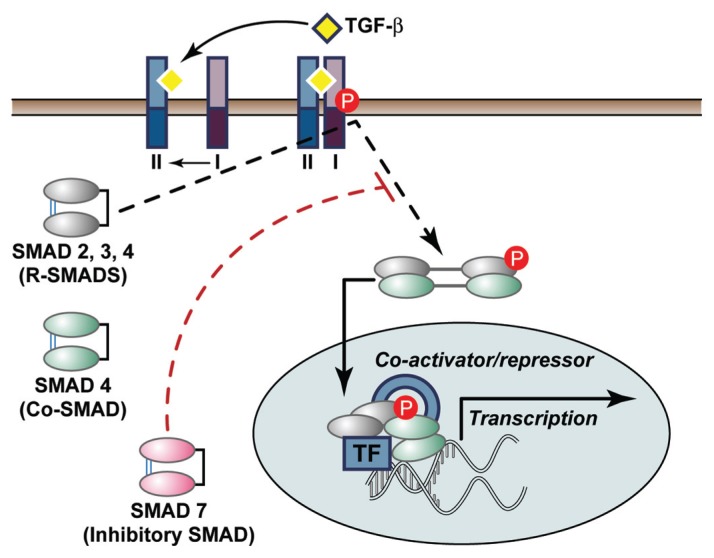
Excessive scars form as a result of aberrations of physiologic wound healing and may arise following any insult to the deep dermis. By causing pain, pruritus and contractures, excessive scarring significantly affects the patient's quality of life, both physically and psychologically. Multiple studies on hypertrophic scar and keloid formation have been conducted for decades and have led to a plethora of therapeutic strategies to prevent or attenuate excessive scar formation. However, most therapeutic approaches remain clinically unsatisfactory, most likely owing to poor understanding of the complex mechanisms underlying the processes of scarring and wound contraction. In this review we summarize the current understanding of the pathophysiology underlying keloid and hypertrophic scar formation and discuss established treatments and novel therapeutic strategies.
Figures
References
-
- Sund B. New Developments in Wound Care. PJB Publications; London: 2000. pp. 1–255.
-
- Berman B, Bieley HC. Keloids. J Am Acad Dermatol. 1995;33:117–23. - PubMed
-
- Peacock EE, Jr, Madden JW, Trier WC. Biologic basis for the treatment of keloids and hypertrophic scars. South Med J. 1970;63:755–60. - PubMed
-
- Mancini RE, Quaife JV. Histogenesis of experimentally produced keloids. J Invest Dermatol. 1962;38:143–81. - PubMed
-
- Atiyeh BS. Nonsurgical management of hypertrophic scars: evidence-based therapies, standard practices, and emerging methods. Aesthetic Plast Surg. 2007;31:468–94. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
