

Cardiovascular magnetic resonance at 3.0 T: current state of the art
- PMID: 20929538
- PMCID: PMC2964699
- DOI: 10.1186/1532-429X-12-55
Cardiovascular magnetic resonance at 3.0 T: current state of the art
Abstract
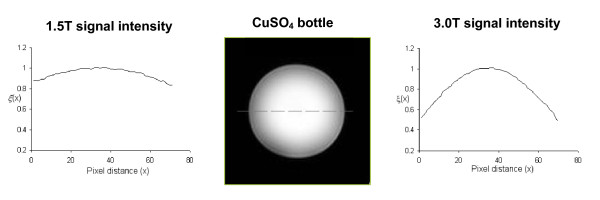
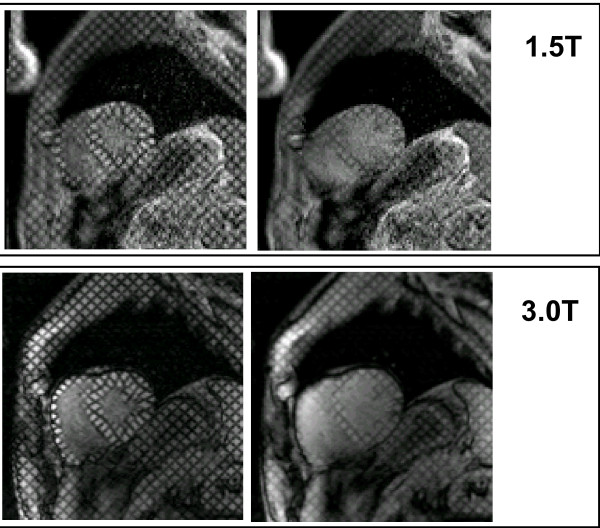
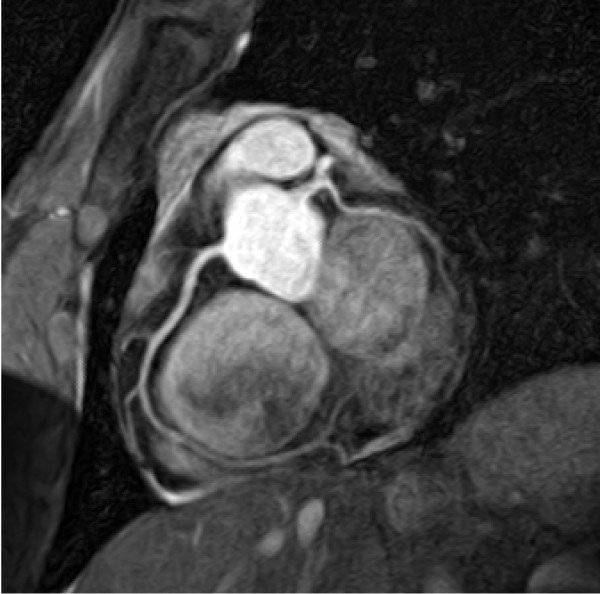
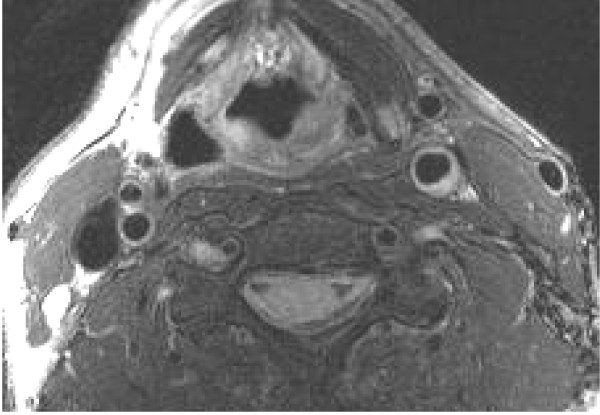
There are advantages to conducting cardiovascular magnetic resonance (CMR) studies at a field strength of 3.0 Telsa, including the increase in bulk magnetization, the increase in frequency separation of off-resonance spins, and the increase in T1 of many tissues. However, there are significant challenges to routinely performing CMR at 3.0 T, including the reduction in main magnetic field homogeneity, the increase in RF power deposition, and the increase in susceptibility-based artifacts.In this review, we outline the underlying physical effects that occur when imaging at higher fields, examine the practical results these effects have on the CMR applications, and examine methods used to compensate for these effects. Specifically, we will review cine imaging, MR coronary angiography, myocardial perfusion imaging, late gadolinium enhancement, and vascular wall imaging.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
