

Pharmacological treatment of the pathogenetic defects in type 2 diabetes: the randomized multicenter South Danish Diabetes Study
- PMID: 20929990
- PMCID: PMC3005476
- DOI: 10.2337/dc10-0531
Pharmacological treatment of the pathogenetic defects in type 2 diabetes: the randomized multicenter South Danish Diabetes Study
Abstract
Objective: To determine the effect of treatment with insulin aspart compared with NPH insulin, together with metformin/placebo and rosiglitazone/placebo. The hypothesis was that combined correction of major pathogenetic defects in type 2 diabetes would result in optimal glycemic control.
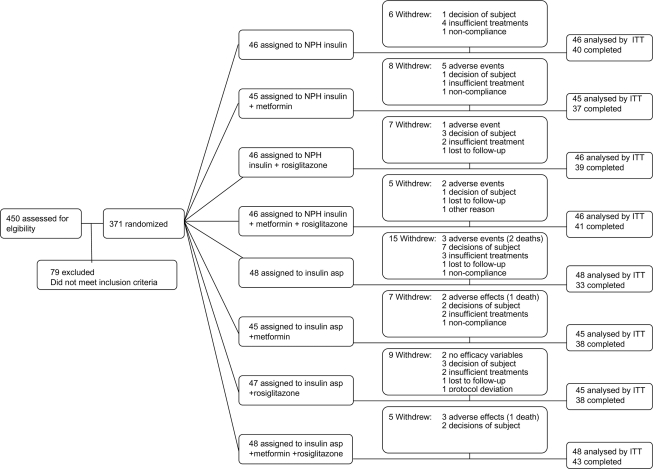
Research design and methods: This study was a 2-year investigator-driven randomized partly placebo-controlled multicenter trial in 371 patients with type 2 diabetes on at least oral antiglycemic treatment. Patients were assigned to one of eight treatment groups in a factorial design with insulin aspart at mealtimes versus NPH insulin once daily at bedtime, metformin twice daily versus placebo, and rosiglitazone twice daily versus placebo. The main outcome measurement was change in A1C.
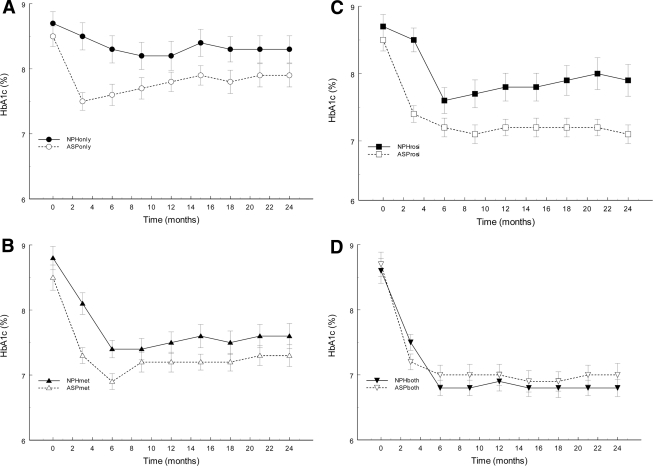
Results: A1C decreased more in patients treated with insulin aspart compared with NPH (-0.41 ± 0.10%, P < 0.001). Metformin decreased A1C compared with placebo (-0.60 ± 0.10%, P < 0.001), as did rosiglitazone (-0.55 ± 0.10%, P < 0.001). Triple therapy (rosiglitazone, metformin, and any insulin) resulted in a greater reduction in A1C than rosiglitazone plus insulin (-0.50 ± 0.14%, P < 0.001) and metformin plus insulin (-0.45 ± 0.14%, P < 0.001). Aspart was associated with a higher increase in body weight (1.6 ± 0.6 kg, P < 0.01) and higher incidence of mild daytime hypoglycemia (4.9 ± 7.5 vs. 1.7 ± 5.4 number/person/year, P < 0.001) compared with NPH.
Conclusions: Insulin treatment of postprandial hyperglycemia results in lower A1C than treatment of fasting hyperglycemia, at the expense of higher body weight and hypoglycemic episodes. However, insulin therapy has to be combined with treatment of both peripheral and liver insulin resistance to normalize blood glucose, and in this case, the insulin regimen is less important.
Figures
References
-
- Nathan DM, Buse JB, Davidson MB, Heine RJ, Holman RR, Sherwin R, Zinman B: Management of hyperglycaemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy. A consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 2006;49:1711–1721 - PubMed
-
- Yki-Jarvinen H, Ryysy L, Nikkila K, Tulokas T, Vanamo R, Heikkila M: Comparison of bedtime insulin regimens in patients with type 2 diabetes mellitus: a randomized, controlled trial. Ann Intern Med 1999;130:389–396 - PubMed
-
- Yki-Jarvinen H, Kauppinen-Makelin R, Tiikkainen M, Vahatalo M, Virtamo H, Nikkila K, Tulokas T, Hulme S, Hardy K, McNulty S, Hanninen J, Levanen H, Lahdenpera S, Lehtonen R, Ryysy L: Insulin glargine or NPH combined with metformin in type 2 diabetes: the LANMET study. Diabetologia 2006;49:442–451 - PubMed
-
- Holman RR, Thorne KI, Farmer AJ, Davies MJ, Keenan JF, Paul S, Levy JC: Addition of biphasic, prandial, or basal insulin to oral therapy in type 2 diabetes. N Engl J Med 2007;357:1716–1730 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
