

Penetration of drugs through the blood-cerebrospinal fluid/blood-brain barrier for treatment of central nervous system infections
- PMID: 20930076
- PMCID: PMC2952976
- DOI: 10.1128/CMR.00007-10
Penetration of drugs through the blood-cerebrospinal fluid/blood-brain barrier for treatment of central nervous system infections
Abstract
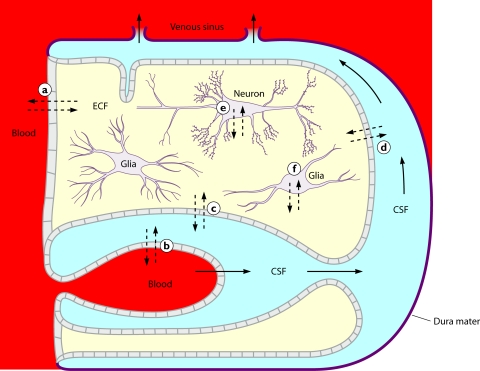
The entry of anti-infectives into the central nervous system (CNS) depends on the compartment studied, molecular size, electric charge, lipophilicity, plasma protein binding, affinity to active transport systems at the blood-brain/blood-cerebrospinal fluid (CSF) barrier, and host factors such as meningeal inflammation and CSF flow. Since concentrations in microdialysates and abscesses are not frequently available for humans, this review focuses on drug CSF concentrations. The ideal compound to treat CNS infections is of small molecular size, is moderately lipophilic, has a low level of plasma protein binding, has a volume of distribution of around 1 liter/kg, and is not a strong ligand of an efflux pump at the blood-brain or blood-CSF barrier. When several equally active compounds are available, a drug which comes close to these physicochemical and pharmacokinetic properties should be preferred. Several anti-infectives (e.g., isoniazid, pyrazinamide, linezolid, metronidazole, fluconazole, and some fluoroquinolones) reach a CSF-to-serum ratio of the areas under the curves close to 1.0 and, therefore, are extremely valuable for the treatment of CNS infections. In many cases, however, pharmacokinetics have to be balanced against in vitro activity. Direct injection of drugs, which do not readily penetrate into the CNS, into the ventricular or lumbar CSF is indicated when other effective therapeutic options are unavailable.
Figures
References
-
- Agwuh, K. N., and A. MacGowan. 2006. Pharmacokinetics and pharmacodynamics of the tetracyclines including glycylcyclines. J. Antimicrob. Chemother. 58:256-265. - PubMed
-
- Albanese, J., M. Leone, B. Bruguerolle, M. L. Ayem, B. Lacarelle, and C. Martin. 2000. Cerebrospinal fluid penetration and pharmacokinetics of vancomycin administered by continuous infusion to mechanically ventilated patients in an intensive care unit. Antimicrob. Agents Chemother. 44:1356-1358. - PMC - PubMed
-
- Albert, F., G. B. Bishop-Freudling, and H. Vergin. 1984. Diffusion of tetroxoprim and sulfadiazine in the cerebrospinal fluid of neurosurgery patients. Fortschr. Med. 102:1064-1066. (In German.) - PubMed
-
- Alffenaar, J. W., R. van Altena, H. J. Bokkerink, G. J. Luijckx, D. van Soolingen, R. E. Aarnoutse, and T. S. van der Werf. 2009. Pharmacokinetics of moxifloxacin in cerebrospinal fluid and plasma in patients with tuberculous meningitis. Clin. Infect. Dis. 49:1080-1082. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
