

One-year costs associated with cardiovascular disease in Canada: Insights from the REduction of Atherothrombosis for Continued Health (REACH) registry
- PMID: 20931098
- PMCID: PMC2954538
- DOI: 10.1016/s0828-282x(10)70437-2
One-year costs associated with cardiovascular disease in Canada: Insights from the REduction of Atherothrombosis for Continued Health (REACH) registry
Abstract
Background and objectives: To provide a contemporary estimate of the economic burden of atherothrombosis in Canada, annual cardiovascular-related hospitalizations, medication use and associated costs across the entire spectrum of atherothrombotic disease were examined.
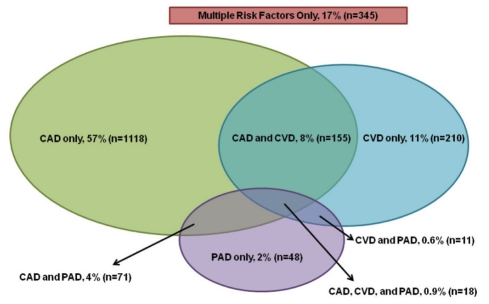
Methods: The REduction of Atherothrombosis for Continued Health (REACH) registry enrolled 1964 Canadian outpatients with coronary artery disease, cerebrovascular disease or peripheral arterial disease (PAD), or three or more cardiovascular risk factors. Baseline data on cardiovascular risk factors and associated medication use, and one-year follow-up data on cardiovascular events, hospitalizations, procedures and medication use were collected. Annual hospitalization and medication costs (Canadian dollars) were derived and compared among patients according to the presence of established atherothrombotic disease at baseline, specific arterial beds affected and the number of affected arterial beds.
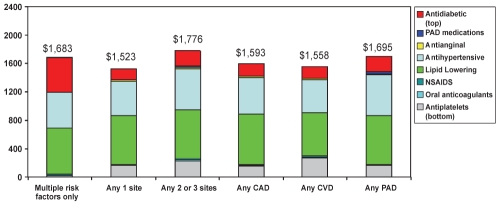
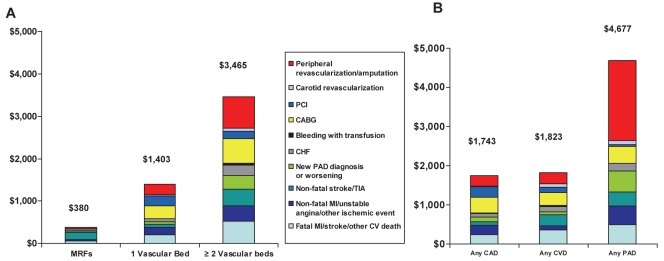
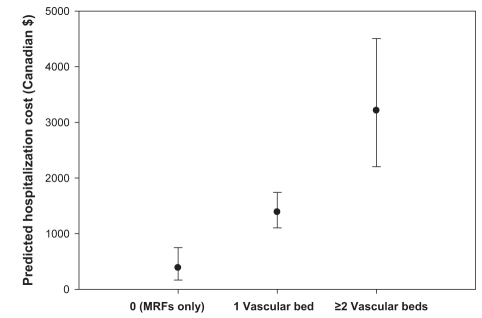
Results: Average annualized medication costs were $1,683, $1,523 and $1,776 for patients with zero, one, and two or three symptomatic arterial beds, respectively. Average annual hospitalization costs increased significantly with the number of beds affected ($380, $1,403 and $3,465, respectively; P<0.0001 for overall linear trend). Mean hospitalization costs for patients with any coronary artery disease, any cerebrovascular disease and any PAD were $1,743, $1,823 and $4,677, respectively. After adjusting for other clinical factors, PAD at baseline was independently associated with a significant increase in hospitalization costs.
Conclusion: Costs associated with vascular-related hospitalizations and interventions for Canadian patients increased with the number of affected arterial beds, and were particularly high for patients with PAD and⁄or polyvascular disease. These contemporary data provide insight into the economic burden associated with atherothrombotic disease in Canada, and highlight the need for increased preventive strategies to lessen the burden for patients and society.
HISTORIQUE ET OBJECTIFS :: Pour fournir une évaluation contemporaine du fardeau économique de l’athérothrombose au Canada, les chercheurs ont examiné les hospitalisations annuelles liées aux troubles cardiovasculaires, l’utilisation de médicaments et les coûts connexes dans tout le spectre des maladies athérothrombotiques.
MÉTHODOLOGIE :: Mille neuf cent soixante-quatre patients externes canadiens ayant une coronaropathie, une maladie cérébrovasculaire ou une maladie artérielle périphérique (MAP) ou au moins trois facteurs de risque cardiovasculaires ont participé au registre REACH pour réduire l’athérothrombose afin de profiter d’une santé constante. Les chercheurs ont colligé les données de départ sur les facteurs de risque cardiovasculaires et l’utilisation connexe de médicaments ainsi que les données de suivi d’un an sur les événements cardiovasculaires, les hospitalisations, les interventions et l’utilisation de médicaments. Ils ont dérivé les coûts annuels d’hospitalisation et des médicaments (en dollars canadiens) et les ont comparés entre patients selon la présence d’une maladie athérothrombotique diagnostiquée au départ, les lits artériels touchés exacts et le nombre de lits artériels touchés.
RÉSULTATS :: Le coût moyen annualisé des médicaments s’élevait à 1 683 $, 1 523 $ et 1 776 $ pour les patients ayant zéro, un et deux ou trois lits artériels symptomatiques, respectivement. Le coût d’hospitalisation annuel moyen a augmentait considérablement, selon le nombre de lits touchés (380 $, 1 403 $ et 3 465 $, respectivement; P<0,0001 pour la tendance linéaire globale). Le coût moyen d’hospitalisation des patients ayant une coronaropathie, une maladie cérébrovasculaire ou une MAP s’élevait à 1 743 $, 1 823 $ et 4 677 $, respectivement. Après rajustement compte tenu d’autres facteurs cliniques, la MAP au départ s’associait de manière indépendante à une augmentation considérable des coûts d’hospitalisation.
CONCLUSION :: Les coûts associés aux hospitalisations et aux interventions découlant de problèmes vasculaires chez les patients canadiens augmentaient selon le nombre de lits artériels touchés et se révélaient particulièrement élevés chez les patients ayant une MAP ou une maladie polyvasculaire. Ces données contemporaines donnent un aperçu du fardeau économique associé à la maladie athérothrombotique au Canada et font ressortir la nécessité d’accroître les stratégies de prévention en vue de réduire le fardeau pour les patients et la société.
Figures
Similar articles
-
One-year costs in patients with a history of or at risk for atherothrombosis in the United States.Circ Cardiovasc Qual Outcomes. 2008 Sep;1(1):38-45. doi: 10.1161/CIRCOUTCOMES.108.775247. Circ Cardiovasc Qual Outcomes. 2008. PMID: 20031786
-
The economic implications of treating atherothrombotic disease in Australia, from the government perspective.Clin Ther. 2010 Jan;32(1):119-32; discussion 106-7. doi: 10.1016/j.clinthera.2010.01.009. Clin Ther. 2010. PMID: 20171418
-
One-year cardiovascular event rates in outpatients with atherothrombosis.JAMA. 2007 Mar 21;297(11):1197-206. doi: 10.1001/jama.297.11.1197. JAMA. 2007. PMID: 17374814
-
The burden of peripheral artery disease and the role of antiplatelet therapy.Postgrad Med. 2009 Jul;121(4):123-35. doi: 10.3810/pgm.2009.07.2038. Postgrad Med. 2009. PMID: 19641278 Review.
-
Lessons from the REACH Registry in Europe.Curr Vasc Pharmacol. 2012 Nov;10(6):725-7. doi: 10.2174/157016112803520774. Curr Vasc Pharmacol. 2012. PMID: 23259566 Review.
Cited by
-
Focus on Prevention: Peripheral Arterial Disease and the Central Role of the Cardiologist.J Clin Med. 2023 Jun 28;12(13):4338. doi: 10.3390/jcm12134338. J Clin Med. 2023. PMID: 37445373 Free PMC article. Review.
-
Genetic Testing for Familial Hypercholesterolemia: Health Technology Assessment.Ont Health Technol Assess Ser. 2022 Aug 23;22(3):1-155. eCollection 2022. Ont Health Technol Assess Ser. 2022. PMID: 36158868 Free PMC article.
-
Below-the-ankle arterial disease: a new marker of coronary artery disease in patients with diabetes and foot ulcers.Acta Diabetol. 2022 Oct;59(10):1331-1338. doi: 10.1007/s00592-022-01932-w. Epub 2022 Jul 21. Acta Diabetol. 2022. PMID: 35864261
-
Outcomes of Hospitalized Patients Undergoing Endoscopic Retrograde Cholangiopancreatography (ERCP) With and Without a History of Peripheral Artery Disease.Cureus. 2022 Jul 5;14(7):e26585. doi: 10.7759/cureus.26585. eCollection 2022 Jul. Cureus. 2022. PMID: 35936117 Free PMC article.
-
Burden of cardiovascular disease attributed to air pollution: a systematic review.Global Health. 2024 May 3;20(1):37. doi: 10.1186/s12992-024-01040-0. Global Health. 2024. PMID: 38702798 Free PMC article.
References
-
- Statistics Canada. Mortality Summary List of Causes. Ottawa: Statistics Canada; 2005. 2009.
-
- Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics – 2009 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:480–6. - PubMed
-
- Allender S, Scarborough P, Peto V, et al. European cardiovascular disease statistics 2008. Brussels: European Heart Network; 2008.
-
- Campbell NR, Tu K, Brant R, Duong-Hua M, McAlister FA. The impact of the Canadian Hypertension Education Program on antihypertensive prescribing trends. Hypertension. 2006;47:22–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
