

Genome profiling of ERBB2-amplified breast cancers
- PMID: 20932292
- PMCID: PMC2958950
- DOI: 10.1186/1471-2407-10-539
Genome profiling of ERBB2-amplified breast cancers
Abstract
Background: Around 20% of breast cancers (BC) show ERBB2 gene amplification and overexpression of the ERBB2 tyrosine kinase receptor. They are associated with a poor prognosis but can benefit from targeted therapy. A better knowledge of these BCs, genomically and biologically heterogeneous, may help understand their behavior and design new therapeutic strategies.
Methods: We defined the high resolution genome and gene expression profiles of 54 ERBB2-amplified BCs using 244K oligonucleotide array-comparative genomic hybridization and whole-genome DNA microarrays. Expression of ERBB2, phosphorylated ERBB2, EGFR, IGF1R and FOXA1 proteins was assessed by immunohistochemistry to evaluate the functional ERBB2 status and identify co-expressions.
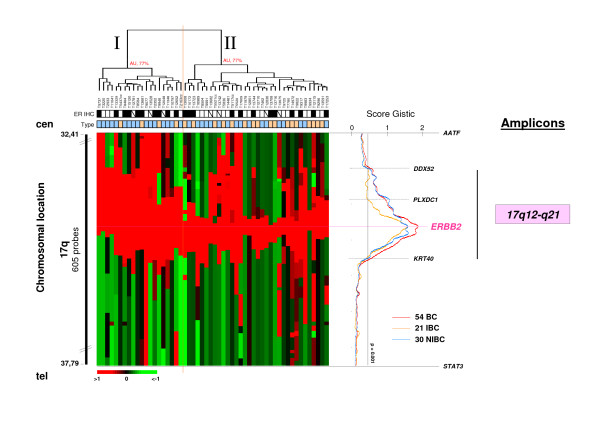
Results: First, we identified the ERBB2-C17orf37-GRB7 genomic segment as the minimal common 17q12-q21 amplicon, and CRKRS and IKZF3 as the most frequent centromeric and telomeric amplicon borders, respectively. Second, GISTIC analysis identified 17 other genome regions affected by copy number aberration (CNA) (amplifications, gains, losses). The expression of 37 genes of these regions was deregulated. Third, two types of heterogeneity were observed in ERBB2-amplified BCs. The genomic profiles of estrogen receptor-positive (ER+) and negative (ER-) ERBB2-amplified BCs were different. The WNT/β-catenin signaling pathway was involved in ER- ERBB2-amplified BCs, and PVT1 and TRPS1 were candidate oncogenes associated with ER+ ERBB2-amplified BCs. The size of the ERBB2 amplicon was different in inflammatory (IBC) and non-inflammatory BCs. ERBB2-amplified IBCs were characterized by the downregulated and upregulated mRNA expression of ten and two genes in proportion to CNA, respectively. IHC results showed (i) a linear relationship between ERBB2 gene amplification and its gene and protein expressions with a good correlation between ERBB2 expression and phosphorylation status; (ii) a potential signaling cross-talk between EGFR or IGF1R and ERBB2, which could influence response of ERBB2-positive BCs to inhibitors. FOXA1 was frequently coexpressed with ERBB2 but its expression did not impact on the outcome of patients with ERBB2-amplified tumors.
Conclusion: We have shown that ER+ and ER- ERBB2-amplified BCs are different, distinguished ERBB2 amplicons in IBC and non-IBC, and identified genomic features that may be useful in the design of alternative therapeutical strategies.
Figures




References
-
- Chin K, DeVries S, Fridlyand J, Spellman PT, Roydasgupta R, Kuo WL, Lapuk A, Neve RM, Qian Z, Ryder T, Chen F, Feiler H, Tokuyasu T, Kingsley C, Dairkee S, Meng Z, Chew K, Pinkel D, Jain A, Ljung BM, Esserman L, Albertson DG, Waldman FM, Gray JW. Genomic and transcriptional aberrations linked to breast cancer pathophysiologies. Cancer Cell. 2006;10:529–541. - PubMed
-
- Letessier A, Sircoulomb F, Ginestier C, Cervera N, Monville F, Gelsi-Boyer V, Esterni B, Geneix J, Finetti P, Zemmour C, Viens P, Charafe-Jauffret E, Jacquemier J, Birnbaum D, Chaffanet M. Frequency, prognosis impact and subtype association of 8p12, 8q24, 11q13, 12p13, 17q12 and 20q13 amplifications in breast cancers. BMC Cancer. 2006;6:245. - PMC - PubMed
-
- Adélaïde J, Finetti P, Bekhouche I, Repellini L, Geneix J, Sircoulomb F, Charafe-Jauffret E, Cervera N, Desplans J, Parzy D, Schoenmakers E, Viens P, Jacquemier J, Birnbaum D, Bertucci F, Chaffanet M. Integrated profiling of basal and luminal breast cancers. Cancer Res. 2007;67:11565–11575. - PubMed
-
- Konecny GE, Pegram MD, Venkatesan N, Finn R, Yang G, Rahmeh M, Untch M, Rusnak DW, Spehar G, Mullin RJ, Keith BR, Gilmer TM, Berger M, Podratz KC, Slamon DJ. Activity of the dual kinase inhibitor lapatinib (GW572016) against HER-2-overexpressing and trastuzumab-treated breast cancer cells. Cancer Res. 2006;66:1630–639. - PubMed
-
- Shepard HM, Jin P, Slamon DJ, Pirot Z, Maneval DC. Herceptin. Handb Exp Pharmacol. 2008;181:183–219. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
