

Laparoscopic enterolithotomy is a valid option to treat gallstone ileus
- PMID: 20932386
- PMCID: PMC3043585
- DOI: 10.4293/108680810X12785289144764
Laparoscopic enterolithotomy is a valid option to treat gallstone ileus
Abstract
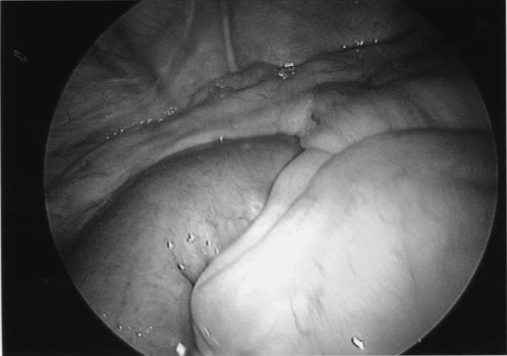
Gallstone ileus is a well-recognized clinical entity. It usually affects elderly female patients, and very often diagnosis can be delayed resulting in high morbidity and mortality. An abdominal x-ray and computed tomographic (CT) scan of the abdomen may show classical radiological features of small bowel obstruction, pneumobilia, and an ectopic gallstone. Laparotomy and enterlithotomy with or without definite biliary surgery is an established treatment. Since 1992, many cases of laparoscopic-assisted enterolithotomy have been reported. Only a few cases of a totally laparoscopic approach have been documented. We present the case of a 75-year-old lady who presented with features of intestinal obstruction. A plain x-ray of the abdomen and a CT scan confirmed the classical features of gallstone ileus. A totally laparoscopic enterolithotomy was performed using 6 ports. A 6-cm gallstone was retrieved through a longitudinal enterotomy. The transverse closure of the enterotomy was performed with intracorporeal suturing, resulting in an uneventful postoperative recovery. We suggest that a CT scan helps in the early diagnosis of the cause of intestinal obstruction, and totally laparoscopic enterolithomy with intracorporeal enterotomy repair is a valid, safe option.
Figures






Similar articles
-
Gallstone ileus with jejunum perforation managed with laparoscopic-assisted surgery: rare case report and minimal invasive management.Int Surg. 2015 May;100(5):878-81. doi: 10.9738/INTSURG-D-14-00265.1. Int Surg. 2015. PMID: 26011209 Free PMC article.
-
Totally laparoscopic management of gallstone ileus--technical report and review of the literature.J Laparoendosc Adv Surg Tech A. 2012 Apr;22(3):265-8. doi: 10.1089/lap.2011.0375. Epub 2012 Feb 3. J Laparoendosc Adv Surg Tech A. 2012. PMID: 22303929 Review.
-
Laparoscopic surgery for gallstone ileus.BMJ Case Rep. 2025 Jan 8;18(1):e263628. doi: 10.1136/bcr-2024-263628. BMJ Case Rep. 2025. PMID: 39778961
-
Gallstone ileus. A case treated with minilaparotomy and a review of the literature.Ann Ital Chir. 2017 Mar 29;6:S2239253X1702535X. Ann Ital Chir. 2017. PMID: 28401880 Review.
-
Gallstone ileus managed with enterolithotomy.BMJ Case Rep. 2019 Oct 13;12(10):e231581. doi: 10.1136/bcr-2019-231581. BMJ Case Rep. 2019. PMID: 31611228 Free PMC article.
Cited by
-
Gall stone ileus: Unfamiliar cause of bowel obstruction. Case report and literature review.Int J Surg Case Rep. 2018;49:44-50. doi: 10.1016/j.ijscr.2018.06.010. Epub 2018 Jun 25. Int J Surg Case Rep. 2018. PMID: 29960209 Free PMC article.
-
Gallstone Ileus Post-cholecystectomy: A Case Review.Cureus. 2023 Jan 4;15(1):e33345. doi: 10.7759/cureus.33345. eCollection 2023 Jan. Cureus. 2023. PMID: 36741674 Free PMC article.
-
Gallstone ileus associated with impaction at Meckel's diverticulum: Case report and literature review.World J Gastrointest Surg. 2016 Nov 27;8(11):755-760. doi: 10.4240/wjgs.v8.i11.755. World J Gastrointest Surg. 2016. PMID: 27933137 Free PMC article.
-
Laparoscopic management for gallstone ileus, case report.Int J Surg Case Rep. 2018;51:268-271. doi: 10.1016/j.ijscr.2018.09.004. Epub 2018 Sep 10. Int J Surg Case Rep. 2018. PMID: 30227374 Free PMC article.
-
Gallstone ileus displaying the typical Rigler triad and an occult second ectopic stone: A case report.Medicine (Baltimore). 2017 Nov;96(45):e8541. doi: 10.1097/MD.0000000000008541. Medicine (Baltimore). 2017. PMID: 29137063 Free PMC article.
References
-
- Reisner RM, Cohen JR. Gallstone ileus: a review of 1001 reported cases. Am Surg. 1994;60:441–446 - PubMed
-
- Patel VG, Gonzales JJ, Fortson JK, Weaver WL. Laparoscopic management of gallstone ileus. Am Surg. 2009;75(1):84–86 - PubMed
-
- El-Dhuwaib Y, Ammori BJ. Staged and complete laparoscopic management of cholelithiasis in a patient with gallstone ileus and bile duct calculi. Surg Endosc. 2003;17(6):988–989;Epub 2003 Mar 14 - PubMed
-
- Rigler LG, Borman CN, Noble JF. Gallstone obstruction. Pathogenesis and roentgen manifestations. JAMA. 1941;117:1753–1759
-
- Tan YM, Wong WK, Ooi LLPJ. A comparison of two surgical strategies for the emergency treatment of gallstone ileus. Singapore Med J. 2004;45:69–72 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources