

Upper airway structure and body fat composition in obese children with obstructive sleep apnea syndrome
- PMID: 20935105
- PMCID: PMC3081285
- DOI: 10.1164/rccm.201008-1249OC
Upper airway structure and body fat composition in obese children with obstructive sleep apnea syndrome
Abstract
Rationale: Mechanisms leading to obstructive sleep apnea syndrome (OSAS) in obese children are not well understood.
Objectives: The aim of the study was to determine anatomical risk factors associated with OSAS in obese children as compared with obese control subjects without OSAS.
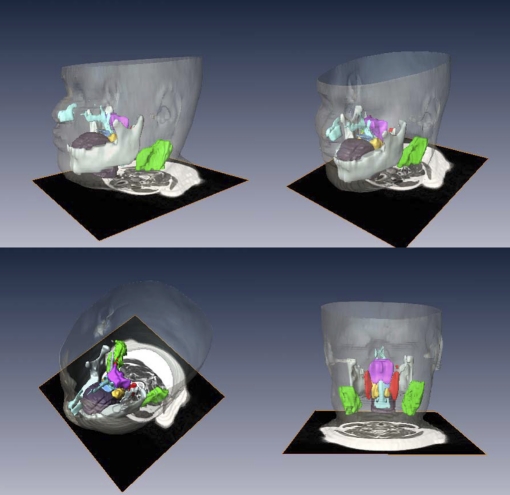
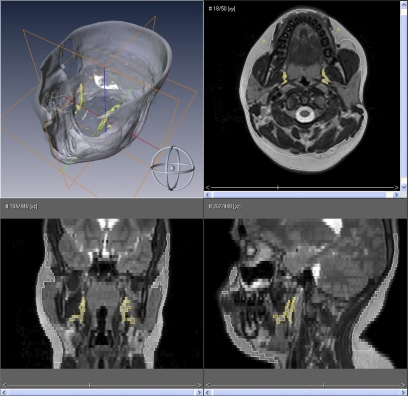
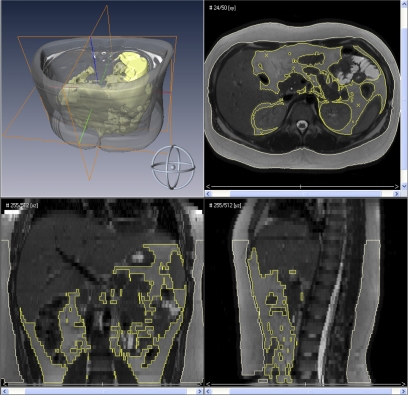
Methods: Magnetic resonance imaging was used to determine the size of upper airway structure, and body fat composition. Paired analysis was used to compare between groups. Mixed effects regression models and conditional multiple logistic regression models were used to determine whether body mass index (BMI) Z-score was an effect modifier of each anatomic characteristic as it relates to OSAS.
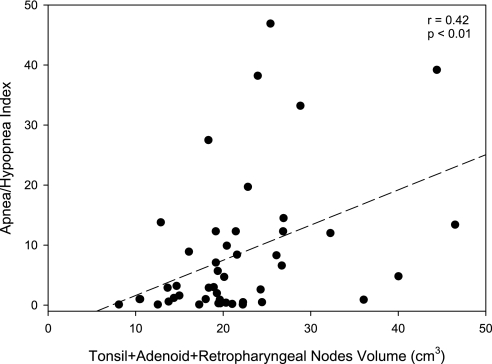
Measurements and main results: We studied 22 obese subjects with OSAS (12.5 ± 2.8 yr; BMI Z-score, 2.4 ± 0.4) and 22 obese control subjects (12.3 ± 2.9 yr; BMI Z-score, 2.3 ± 0.3). As compared with control subjects, subjects with OSAS had a smaller oropharynx (P < 0.05) and larger adenoid (P < 0.01), tonsils (P < 0.05), and retropharyngeal nodes (P < 0.05). The size of lymphoid tissues correlated with severity of OSAS whereas BMI Z-score did not have a modifier effect on these tissues. Subjects with OSAS demonstrated increased size of parapharyngeal fat pads (P < 0.05) and abdominal visceral fat (P < 0.05). The size of these tissues did not correlate with severity of OSAS and BMI Z-score did not have a modifier effect on these tissues.
Conclusions: Upper airway lymphoid hypertrophy is significant in obese children with OSAS. The lack of correlation of lymphoid tissue size with obesity suggests that this hypertrophy is caused by other mechanisms. Although the parapharyngeal fat pads and abdominal visceral fat are larger in obese children with OSAS we could not find a direct association with severity of OSAS or with obesity.
Figures
Comment in
-
Fat and lymphadenoid tissues: a mutually obstructive combination.Am J Respir Crit Care Med. 2011 Mar 15;183(6):694-5. doi: 10.1164/rccm.201010-1681ED. Am J Respir Crit Care Med. 2011. PMID: 21471065 No abstract available.
-
Upper airway lymphoid tissues in obese children with sleep apnea: clinical implications.Am J Respir Crit Care Med. 2011 Apr 1;183(7):950-1; author reply 951-2. doi: 10.1164/ajrccm.183.7.950b. Am J Respir Crit Care Med. 2011. PMID: 21471078 No abstract available.
References
-
- Redline S, Tishler PV, Schluchter M, Aylor J, Clark K, Graham G. Risk factors for sleep-disordered breathing in children: associations with obesity, race, and respiratory problems. Am J Respir Crit Care Med 1999;159:1527–1532. - PubMed
-
- Marcus CL, Curtis S, Koerner CB, Joffe A, Serwint JR, Loughlin GM. Evaluation of pulmonary function and polysomnography in obese children and adolescents. Pediatr Pulmonol 1996;21:176–183. - PubMed
-
- Kalra M, Inge T, Garcia V, Daniels S, Lawson L, Curti R, Cohen A, Amin R. Obstructive sleep apnea in extremely overweight adolescents undergoing bariatric surgery. Obes Res 2005;13:1175–1179. - PubMed
-
- Silvestri JM, Weese-Mayer DE, Bass MT, Kenny AS, Hauptman SA, Pearsall SM. Polysomnography in obese children with a history of sleep-associated breathing disorders. Pediatr Pulmonol 1993;16:124–129. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
