

Cardiorespiratory instability before and after implementing an integrated monitoring system
- PMID: 20935559
- PMCID: PMC3673290
- DOI: 10.1097/CCM.0b013e3181fb7b1c
Cardiorespiratory instability before and after implementing an integrated monitoring system
Abstract
Objectives: Cardiorespiratory instability may be undetected in monitored step-down unit patients. We explored whether using an integrated monitoring system that continuously amalgamates single noninvasive monitoring parameters (heart rate, respiratory rate, blood pressure, and peripheral oxygen saturation) into AN instability index value (INDEX) correlated with our single-parameter cardiorespiratory instability concern criteria, and whether nurse response to INDEX alert for patient attention was associated with instability reduction.
Design: Prospective, longitudinal evaluation in sequential 8-, 16-, and 8-wk phases (phase I, phase II, and phase III, respectively).
Setting: A 24-bed trauma step-down unit in single urban tertiary care center.
Patients: All monitored patients.
Interventions: Phase I: Patients received continuous single-channel monitoring (heart rate, respiratory rate, blood pressure, and peripheral oxygen saturation) and standard care; INDEX background was recorded but not displayed. Phase II: INDEX was background-recorded; staff was educated on use. Phase III: Staff used a clinical response algorithm for INDEX alerts.
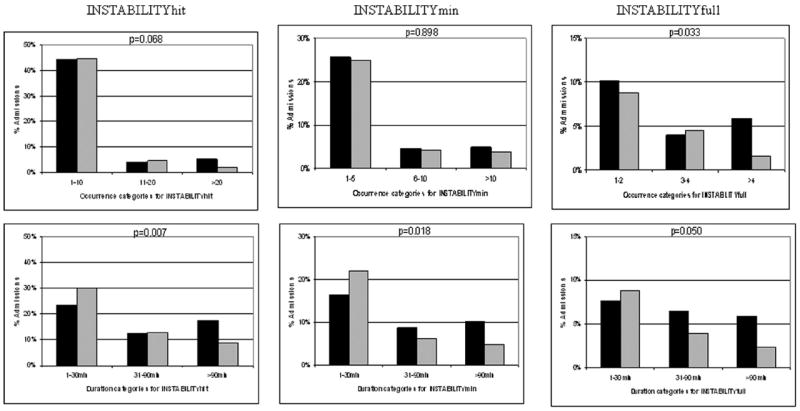
Measurement and main results: Any monitored parameters even transiently beyond local cardiorespiratory instability concern triggers (heart rate of <40 or >140 beats/min, respiratory rate of <8 or >36 breaths/min, systolic blood pressure of <80 or >200 mm Hg, diastolic blood pressure of >110 mm Hg, and peripheral oxygen saturation of <85%) defined INSTABILITYmin. INSTABILITYmin further judged as both persistent and serious defined INSTABILITYfull. The INDEX alert states were defined as INDEXmin and INDEXfull by using same classification. Phase I and phase III admissions (323 vs. 308) and monitoring (18,258 vs. 18,314 hrs) were similar. INDEXmin and INDEXfull correlated significantly with INSTABILITYmin and INSTABILITYfull (r = .713 and r = .815, respectively, p < .0001). INDEXmin occurred before INSTABILITYmin in 80% of cases (mean advance time 9.4 ± 9.2 mins). Phase I and phase III admissions were similarly likely to develop INSTABILITYmin (35% vs. 33%), but INSTABILITYmin duration/admission decreased from phase I to phase III (p = .018). Both INSTABILITYfull episodes/admission (p = .03) and INSTABILITYfull duration/admission (p = .05) decreased in phase III.
Conclusion: The integrated monitoring system INDEX correlated significantly with cardiorespiratory instability concern criteria, usually occurred before overt instability, and when coupled with a nursing alert was associated with decreased cardiorespiratory instability concern criteria in step-down unit patients.
Conflict of interest statement
The authors have not disclosed any potential conflicts of interest.
Figures



Comment in
-
Monitoring the ill: Is this another measurement or will it change outcomes?Crit Care Med. 2011 Jan;39(1):202-3. doi: 10.1097/CCM.0b013e3181feb67a. Crit Care Med. 2011. PMID: 21178538 No abstract available.
References
-
- US Department of Health and Human Services, Agency for Healthcare Research and Quality. AHRQ Quality Indicators: Patient Safety Indicators. Rockville, MD: Agency for Healthcare Research and Quality; 2006.
-
- Devita MA, Bellomo R, Hillman K, et al. Findings of the first consensus conference on medical emergency teams. Crit Care Med. 2006;34:2463–2478. - PubMed
-
- Smith GB, Prytherch DR, Schmidt PE. Review and performance evaluation of aggregate weighted ‘track and trigger’ systems. Resuscitation. 2008;77:170–179. - PubMed
-
- Subbe CP, Kruger M, Rutherford P, et al. Validation of a modified Early Warning Score in medical admissions. QJM. 2001;94:521–526. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
