

Anatomy of the psoas muscle and lumbar plexus with respect to the surgical approach for lateral transpsoas interbody fusion
- PMID: 20938787
- PMCID: PMC3065600
- DOI: 10.1007/s00586-010-1593-5
Anatomy of the psoas muscle and lumbar plexus with respect to the surgical approach for lateral transpsoas interbody fusion
Abstract
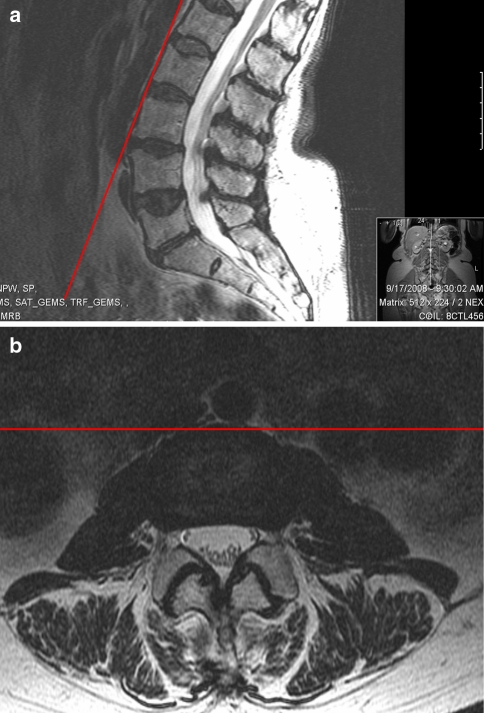
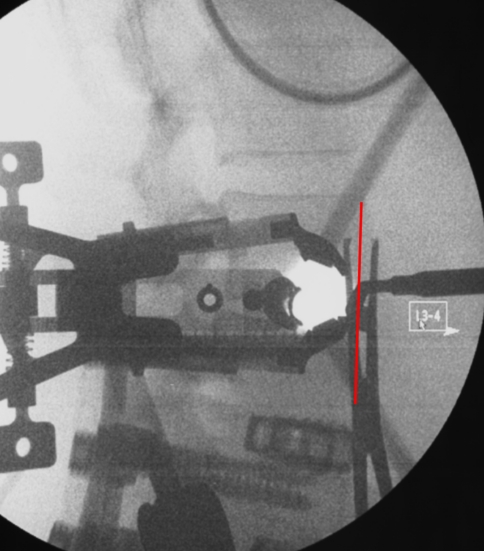
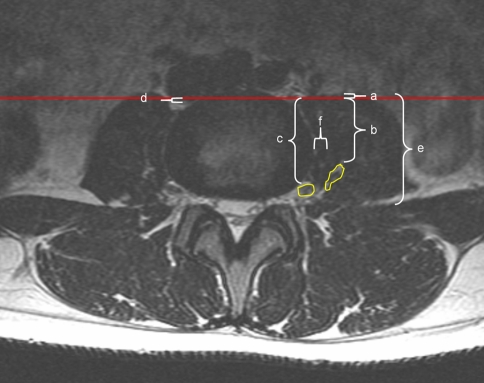
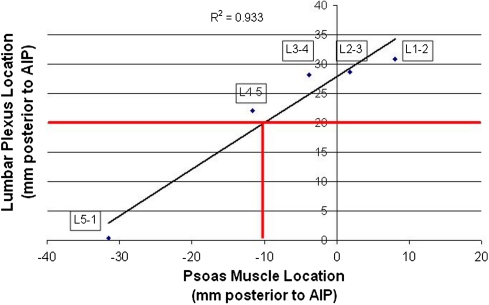
Lateral transpsoas interbody fusion (LTIF) is a minimally invasive technique that permits interbody fusion utilizing cages placed via a direct lateral retroperitoneal approach. We sought to describe the locations of relevant neurovascular structures based on MRI with respect to this novel surgical approach. We retrospectively reviewed consecutive lumbosacral spine MRI scans in 43 skeletally mature adults. MRI scans were independently reviewed by two readers to identify the location of the psoas muscle, lumbar plexus, femoral nerve, inferior vena cava and right iliac vein. Structures potentially at risk for injury were identified by: a distance from the anterior aspect of the adjacent vertebral bodies of <20 mm, representing the minimum retraction necessary for cage placement, and extension of vascular structures posterior to the anterior vertebral body, requiring anterior retraction. The percentage of patients with neurovascular structures at risk for left-sided approaches was 2.3% at L1-2, 7.0% at L2-3, 4.7% at L3-4 and 20.9% at L4-5. For right-sided approaches, this rose to 7.0% at L1-2, 7.0% at L2-3, 9.3% at L3-4 and 44.2% at L4-5, largely because of the relatively posterior right-sided vasculature. A relationship between the position of psoas muscle and lumbar plexus is described which allows use of the psoas position as a proxy for lumbar plexus position to identify patients who may be at risk, particularly at the L4-5 level. Further study will establish the clinical relevance of these measurements and the ability of neurovascular structures to be retracted without significant injury.
Figures
References
-
- Kirchmair L, Lirk P, Colvin J, Mitterschiffthaler G, Moriggl B. Lumbar plexus and psoas major muscle: not always as expected. Reg Anesth Pain Med. 2008;33:109–114. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
