

Silent cerebral infarcts occur despite regular blood transfusion therapy after first strokes in children with sickle cell disease
- PMID: 20940417
- PMCID: PMC3035071
- DOI: 10.1182/blood-2010-01-261123
Silent cerebral infarcts occur despite regular blood transfusion therapy after first strokes in children with sickle cell disease
Abstract
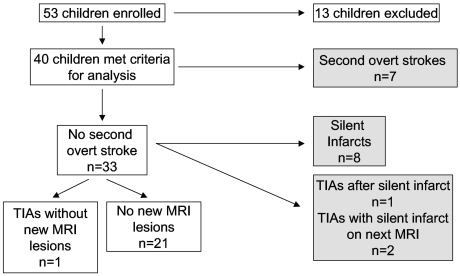
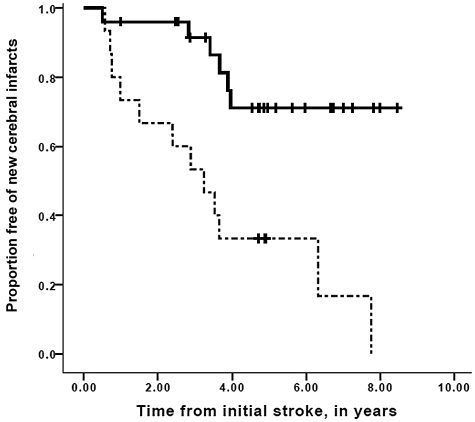
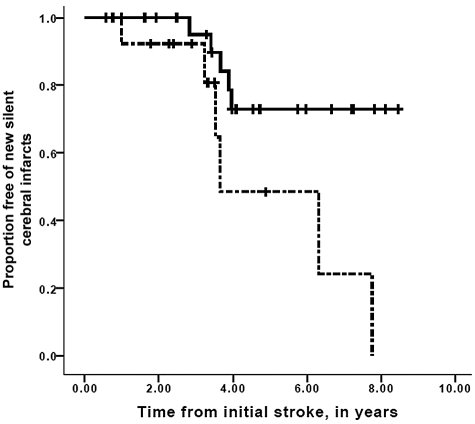
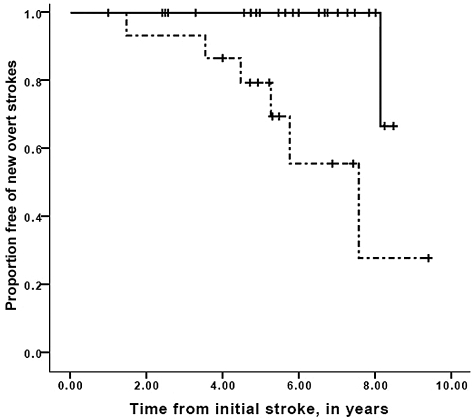
Children with sickle cell disease (SCD) and strokes receive blood transfusion therapy for secondary stroke prevention; despite this, approximately 20% experience second overt strokes. Given this rate of second overt strokes and the clinical significance of silent cerebral infarcts, we tested the hypothesis that silent cerebral infarcts occur among children with SCD being transfused for secondary stroke prevention. A prospective cohort enrolled children with SCD and overt strokes at 7 academic centers. Magnetic resonance imaging and magnetic resonance angiography of the brain were scheduled approximately every 1 to 2 years; studies were reviewed by a panel of neuroradiologists. Eligibility criteria included regularly scheduled blood transfusion therapy. Forty children were included; mean pretransfusion hemoglobin S concentration was 29%. Progressive cerebral infarcts occurred in 45% (18 of 40 children) while receiving chronic blood transfusion therapy; 7 had second overt strokes and 11 had new silent cerebral infarcts. Worsening cerebral vasculopathy was associated with new cerebral infarction (overt or silent; relative risk = 12.7; 95% confidence interval, 2.65-60.5, P = .001). Children with SCD and overt strokes receiving regular blood transfusion therapy experience silent cerebral infarcts at a higher rate than previously recognized. Additional therapies are needed for secondary stroke prevention in children with SCD.
Figures
Comment in
-
So what if blood is thicker than water?Blood. 2011 Jan 20;117(3):745-6. doi: 10.1182/blood-2010-11-314484. Blood. 2011. PMID: 21252094 No abstract available.
References
-
- Ohene-Frempong K, Weiner SJ, Sleeper LA, et al. Cerebrovascular accidents in sickle cell disease: rates and risk factors. Blood. 1998;91(1):288–294. - PubMed
-
- Scothorn DJ, Price C, Schwartz D, et al. Risk of recurrent stroke in children with sickle cell disease receiving blood transfusion therapy for at least five years after initial stroke. J Pediatr. 2002;140(3):48–54. - PubMed
-
- Powars D, Wilson B, Imbus C, Pegelow C, Allen J. The natural history of stroke in sickle cell disease. Am J Med. 1978;65(3):461–471. - PubMed
-
- Pavlakis SG, Bello J, Prohovnik I, et al. Brain infarction in sickle cell anemia: magnetic resonance imaging correlates. Ann Neurol. 1988;23(2):125–130. - PubMed
