

MRSA in a large German University Hospital: Male gender is a significant risk factor for MRSA acquisition
- PMID: 20941335
- PMCID: PMC2951106
- DOI: 10.3205/dgkh000154
MRSA in a large German University Hospital: Male gender is a significant risk factor for MRSA acquisition
Abstract
Background: The continually rising number of hospital acquired infections and particularly MRSA (Methicillin-resistant Staphylococcus aureus) colonization poses a major challenge from both clinical and epidemiological perspectives. The assessment of risk factors is vital in determining the best prevention, diagnosis and treatment strategies.
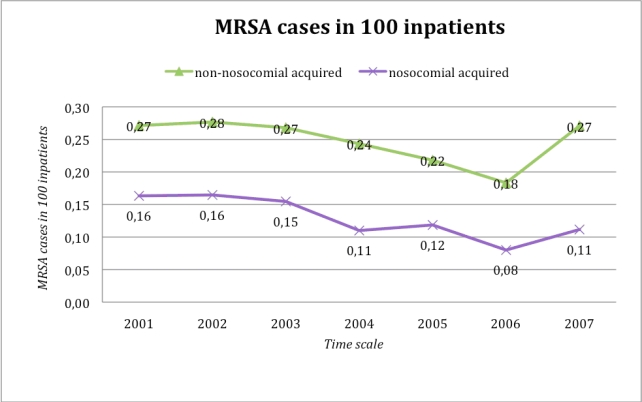
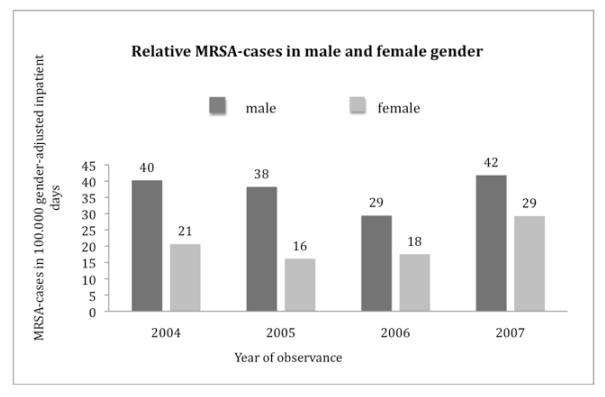
Materials and methods: We analyzed 798 cases of MRSA in a large German University Hospital over a 7-year period. Data was collected retro- and prospectively including patient age, sex, type of ward and duration of inpatient stay. In addition we analyzed all cases on ICU with regards to cross infection and MRSA genotyping via DNA MicroArray Technology. The years 2004 to 2007 were analyzed with a specific focus on gender.
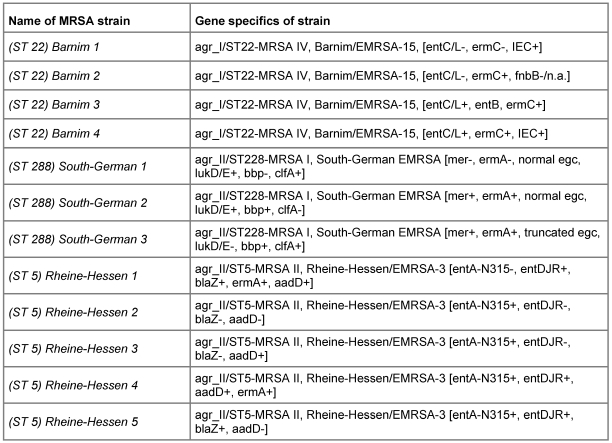
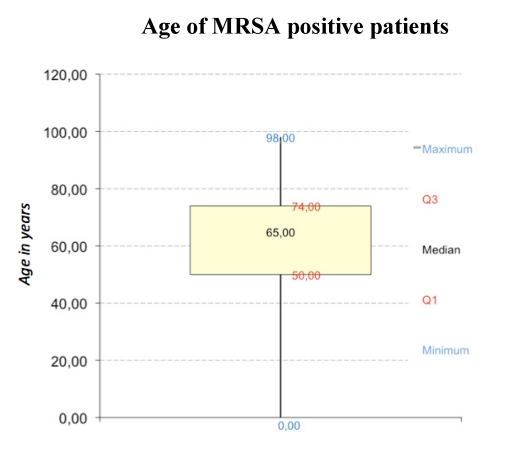
Results: Male gender is significantly correlated with increased risk of MRSA acquisition (p<0.001), the predominant setting for MRSA is on ICU. 75% of the MRSA positive patients are over 50 years of age (average age 59.8 years). The inpatient time was 4.15 times higher in MRSA carriers compared with non-MRSA cases, however this was not significant. MRSA genotyping on ICU showed mainly the subtypes ST 5, ST 22, ST 228, however cross contamination with identical genotypes was only detected in a minority of cases (5 out of 22).
Conclusion: Unlike previous studies which show no or inconclusive evidence of gender as a risk factor, our data confirm that male gender is a significant risk factor for MRSA carrier status. Further research will be required to investigate the aetiology of these findings.
Hintergrund: Die steigende Anzahl von Patienten mit Methicillin resistenten Staphylococcus aureus (MRSA)-Kolonisation oder -Infektion ist unter klinischen, epidemiologischen wie auch ökonomischen Gesichtspunkten ein Problem. Um die Situation des Uniklinikums Dresden (UKD) national einzuordnen, intern zu analysieren und das MRSA-Management weiter zu optimieren, wurde diese Untersuchung durchgeführt.
Methode: In einer retro- und im letzten Jahr der Auswertung prospektiven 7 Jahresstudie (2001 bis 2007) wurden 798 stationäre MRSA-Fälle in Anlehnung an das nationale MRSA-Surveillancesystem MRSA-KISS (Krankenhaus-Infektions-Surveillance-System) erfasst und hinsichtlich Risikofaktoren analysiert. Die Isolate von Patienten der Intensivstationen aus dem Jahr 2007 wurden genotypisiert (Microarray Technology, CLONDIAG®) und Transmissionswege aufgezeigt.
Ergebnisse: Durchschnittlich waren MRSA-Patienten 59,8 Jahre alt und zu 75% älter als 50 Jahre. Eine signifikante (p<0,001) Häufung von MRSA konnte im Bezug auf das männliche Geschlecht herausgestellt werden. Die Verweildauer der MRSA-Patienten war im Vergleich zu Patienten ohne MRSA-Nachweis um den Faktor 4,15 höher. Nicht nosokomiale Fälle (n=385) zeigten im Bezug auf den Aufenthaltsort vor der stationären Aufnahme, dass 62,5% aus ihrer häuslichen Umgebung (nicht Pflegeheime), 26,6% aus medizinischen Einrichtungen und 4,9% aus Pflegeheimen aufgenommen wurden (6% nicht eruierbar). Im nationalen Vergleich mit den MRSA-KISS Referenzdaten ordnet sich das Universitätsklinikum Dresden bezüglich nosokomialer und nicht nosokomialer Inzidenzdichte und MRSA-Last von 2004 bis 2007 jeweils kleiner/gleich des 25%-Quantils ein. Die nosokomialen Fälle pro 1.000 MRSA-Tage sind im nationalen Vergleich über dem 50%-Quantil einzuordnen. Intensivstationen zeigten im klinikinternen Stationsgruppenvergleich die höchsten Inzidenzdichten, die höchste MRSA-Last und die meisten nosokomialen MRSA-Fälle. Die Genotypisierung auf ITS ergab, dass unterschiedliche Epidemiestämme vorkamen (ST 5, ST 22, ST 228). Das Auftreten von genotypisch identischen MRSA konnte in der Minorität der Fälle (5 von 22) nachgewiesen werden.
Schlussfolgerung: Zusätzlich zu den vom Robert-Koch-Institut publizierten Risikofaktoren hat sich in der eigenen Patientenklientel das männliche Geschlecht als signifikanter Risikofaktor darstellt. Die MRSA-Belastung ist im Stationsgruppenvergleich auf den Intensivstationen besonders groß. Aufenthaltsort nicht nosokomialer MRSA-Fälle vor Hospitalisation ist mehrheitlich die häusliche Umgebung. Die durchschnittliche Verweildauer von MRSA-Patienten ist höher als die anderer Patienten. Die Genotypisierung stellt eine sinnvolle Maßnahme dar um die Transmissionskette von MRSA zu verstehen und gezielt Hygienemaßnahmen einzuleiten.
Figures


Similar articles
-
"Colonization pressure" and risk of acquisition of methicillin-resistant Staphylococcus aureus in a medical intensive care unit.Infect Control Hosp Epidemiol. 2000 Nov;21(11):718-23. doi: 10.1086/501721. Infect Control Hosp Epidemiol. 2000. PMID: 11089656
-
Colonization with methicillin-resistant Staphylococcus aureus in ICU patients: morbidity, mortality, and glycopeptide use.Infect Control Hosp Epidemiol. 2001 Nov;22(11):687-92. doi: 10.1086/501846. Infect Control Hosp Epidemiol. 2001. PMID: 11842988
-
Acquisition of methicillin-resistant Staphylococcus aureus in a large intensive care unit.Infect Control Hosp Epidemiol. 2003 May;24(5):322-6. doi: 10.1086/502215. Infect Control Hosp Epidemiol. 2003. PMID: 12785404
-
Acquisition and cross-transmission of Staphylococcus aureus in European intensive care units.Infect Control Hosp Epidemiol. 2009 Feb;30(2):117-24. doi: 10.1086/593126. Infect Control Hosp Epidemiol. 2009. PMID: 19133819
-
[Meticillin-resistant Staphylococcus aureus: incidence, risk factors and interest of systematic screening for colonization in intensive-care unit].Ann Fr Anesth Reanim. 2006 Jun;25(6):626-32. doi: 10.1016/j.annfar.2006.01.016. Epub 2006 Mar 20. Ann Fr Anesth Reanim. 2006. PMID: 16546345 Review. French.
Cited by
-
Risk factors for carriage of antimicrobial-resistant bacteria in community dwelling-children in the Asia-Pacific region: a systematic review and meta-analysis.JAC Antimicrob Resist. 2022 Apr 19;4(2):dlac036. doi: 10.1093/jacamr/dlac036. eCollection 2022 Apr. JAC Antimicrob Resist. 2022. PMID: 35449720 Free PMC article. Review.
-
The global prevalence of methicillin-resistant Staphylococcus aureus colonization in residents of elderly care centers: a systematic review and meta-analysis.Antimicrob Resist Infect Control. 2023 Jan 29;12(1):4. doi: 10.1186/s13756-023-01210-6. Antimicrob Resist Infect Control. 2023. PMID: 36709300 Free PMC article.
-
Genotyping of methicillin-resistant Staphylococcus aureus from sepsis patients in Pakistan and detection of antibodies against staphylococcal virulence factors.Eur J Clin Microbiol Infect Dis. 2020 Jan;39(1):85-92. doi: 10.1007/s10096-019-03695-9. Epub 2019 Sep 3. Eur J Clin Microbiol Infect Dis. 2020. PMID: 31482419
-
MRSA Profiles Reveal Age- and Gender-Specificity in a Tertiary Care Hospital: High Burden in ICU Elderly and Emerging Community Patterns in Youth.Microorganisms. 2025 May 6;13(5):1078. doi: 10.3390/microorganisms13051078. Microorganisms. 2025. PMID: 40431251 Free PMC article.
-
Predictors of community-associated Staphylococcus aureus, methicillin-resistant and methicillin-susceptible Staphylococcus aureus skin and soft tissue infections in primary-care settings.Epidemiol Infect. 2016 Nov;144(15):3198-3204. doi: 10.1017/S0950268816001709. Epub 2016 Aug 4. Epidemiol Infect. 2016. PMID: 27489019 Free PMC article.
References
-
- Kipp F, Friedrich AW, Becker K, von Eiff C. Bedrohliche Zunahme Methicillin-resistenter Staphylococcus-aureus-Stämme: Strategien zur Kontrolle und Prävention in Deutschland. Dtsch Arztebl. 2004;101(28-29):2045–2050.
-
- Marcotte AL, Trzeciak MA. Community-acquired methicillin-resistant Staphylococcus aureus: an emerging pathogen in orthopaedics. J Am Acad Orthop Surg. 2008;16(2):98–106. - PubMed
-
- Noskin GA, Rubin RJ, Schentag JJ, Kluytmans J, Hedblom EC, Smulders M, et al. The burden of Staphylococcus aureus infections on hospitals in the United States: an analysis of the 2000 and 2001 Nationwide Inpatient Sample Database. Arch Intern Med. 2005;165(15):1756–1761. doi: 10.1001/archinte.165.15.1756. Available from: http://dx.doi.org/10.1001/archinte.165.15.1756. - DOI - DOI - PubMed
-
- D'Agata EM, Webb GF, Horn MA, Moellering RC, Jr, Ruan S. Modeling the invasion of community-acquired methicillin-resistant Staphylococcus aureus into hospitals. Clin Infect Dis. 2009;48(3):274–284. doi: 10.1086/595844. Available from: http://dx.doi.org/10.1086/595844. - DOI - DOI - PMC - PubMed
-
- Cosgrove SE, Sakoulas G, Perencevich EN, Schwaber MJ, Karchmer AW, Carmeli Y. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: a meta-analysis. Clin Infect Dis. 2003;36(1):53–59. doi: 10.1086/345476. Available from: http://dx.doi.org/10.1086/345476. - DOI - DOI - PubMed
LinkOut - more resources
Full Text Sources
