

Serial testing with an interferon-γ release assay in German healthcare workers
- PMID: 20941341
- PMCID: PMC2951105
- DOI: 10.3205/dgkh000148
Serial testing with an interferon-γ release assay in German healthcare workers
Abstract
Aim: Data concerning conversion and reversion rates in the serial testing of healthcare workers (HCWs) is rare. So far, there is no consensus on how to define and interpret interferon-gamma release assays (IGRA) conversions and reversions, or how to deal with such results. We analysed conversion and reversion rates in the serial testing of HCWs using an IGRA.
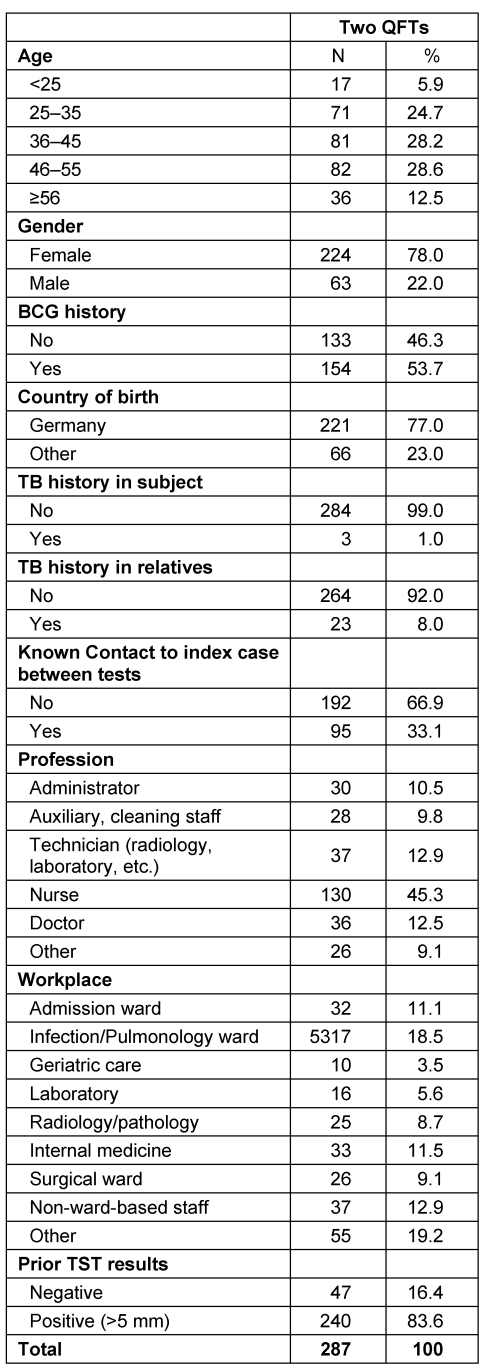
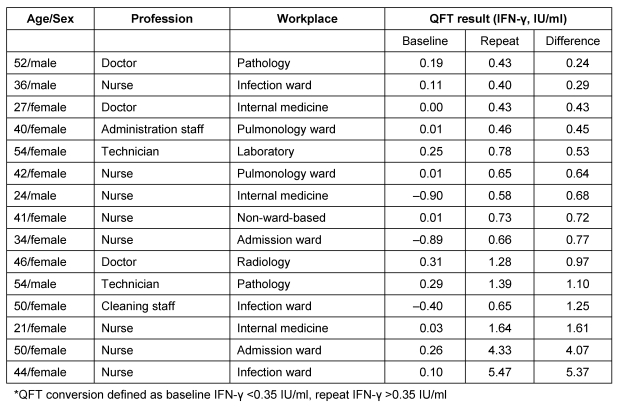
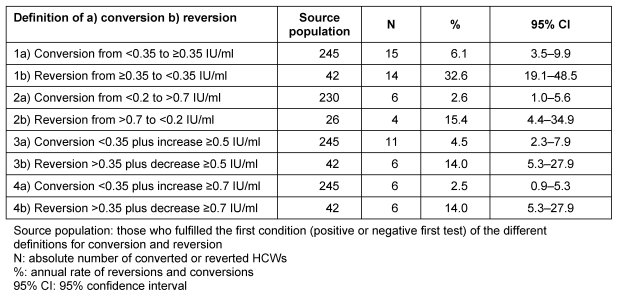
Methods: The study population comprises 287 HCWs, who participated in routine occupational safety and health screening for latent tuberculosis infection (LTBI) with the QuantiFERON-TB(®) Gold In-Tube assay (QFT). Four different definitions for conversion and reversion were applied: 1) transgression or regression above/below the cut-off; 2) increase from <0.2 to >0.7 IU/ml or decrease from >0.7 to <0.2 IU/ml; 3) transgression or regression above/below the cut-off plus change of ≥0.50 IU/ml; and 4) transgression or regression above/below the cut-off plus change of ≥0.70 IU/ml.
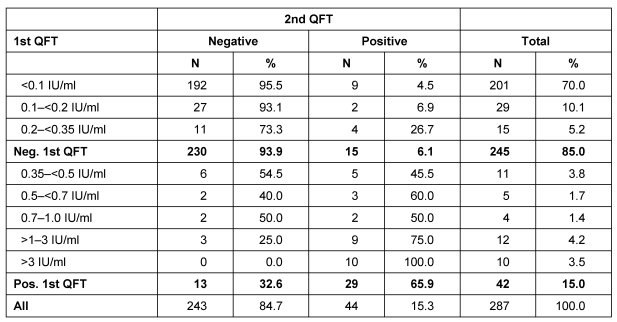
Results: The highest conversion and reversion rates of 6.1% (95% CI 3.5 to 9.9) and 32.6% (95% CI 19.1 to 48.5) respectively were observed with the least stringent definition of negative to positive. The most stringent definition of an increase of ≥0.7 IU/ml above the cut-point produced the lowest conversion rate of 2.5% (95% CI 0.9 to 5.3). Using an uncertainty zone from 0.2 to 0.7 IU/ml gave low conversion (2.6%) and reversion rates (15.4%).
Conclusion: Our data confirmed the findings of previous studies that suggest that a simplistic dichotomous negative to positive definition of the IGRA might be deceptive because of the high number of spontaneous conversions and reversions. Therefore using an uncertainty zone around the cut-point (e.g. 0.2 to 0.7 IU/ml) could improve the discrimination between unspecific variation around the diagnostic cut-off and true conversion or reversion.
Hintergrund: Die neuen Richtlinien zur Diagnose einer Latenten Tuberkulose Infektion (LTBI) bei Beschäftigten im Gesundheitswesen empfehlen den Interferon-gamma Release Assays (IGRA) als Diagnoseinstrument. Trotz wachsender Erfahrung mit dem Test liegen bislang nur wenige Daten zum Seriellen Testen vor. Dies gilt vor allem für Länder mit niedriger LTBI- Prävalenz. Bei wiederholten Tests ist bislang unklar, ab wann von wahren „Konversionen und Reversionen“ auszugehen ist, wie diese interpretiert werden sollen und wann eine Chemoprävention indiziert ist. Wir haben in unserer Studie Konversions- und Reversionsraten bei Beschäftigten im Gesundheitsdienst analysiert.
Methode: Insgesamt wurden 287 Beschäftigte im Gesundheitswesen, die routinemäßig arbeitsmedizinisch auf TB untersucht wurden, in die Studie eingeschlossen und zu zwei Zeitpunkten mit dem QuantiFERON-TB Gold In Tube (QFT) untersucht. Vier unterschiedliche Definitionen für Konversionen und Reversionen wurden analysiert. Zusätzlich wurde die Verwendung einer Grauzone um den Grenzwert (0,35 IU/ml) von 0,2–0,7 IU/ml untersucht.
Ergebnisse: Bei 15% der Beschäftigten waren beide Testergebnisse positiv. Die höchsten Konversion (6,1%) und Reversionsraten (32,6%) wurden mit der am wenigsten stringenten Definition von negativ zu positiv beobachtet. Die niedrigsten Raten (2,5%) fanden sich bei der strengsten Definition mit einem Anstieg von ≥0,7 IU/ml über dem Grenzwert von 0,35 IU/ml. Bei der Verwendung einer Grauzone von 0,2–0,7 IU/ml um den Grenzwert lagen die Konversionsrate bei 2,6% und die Reversionsrate bei 15,4%. Bei einem positiven QFT-Test wurde eine Röntgenuntersuchung zum Ausschluss einer aktiven Tuberkulose (TB) durchgeführt. Keiner der Probanden hat bislang eine aktive TB entwickelt.
Schlussfolgerung: Die Konversions- und Reversionsraten variieren in Abhängigkeit der jeweiligen Definition. Unsere Daten bestätigen die Annahme einer Grauzone zwischen 0,2 und 0,7 IU/ml bei wiederholten Routineuntersuchungen von Personen mit einem erhöhten LTBI- Risiko. Dies sollte in einer größeren Studienpopulation evaluiert werden. Zur Progressionsrate eines positiven QFT in Niedrig- Inzidenzländern liegen wenige Daten vor. Deshalb sollten Personen, deren Testergebnisse in diese Grauzone fallen vor Beginn einer Chemoprävention nochmals mit dem QFT untersucht werden.
Keywords: healthcare workers; interferon-gamma release assay; latent TB infection; serial testing.
Figures
Similar articles
-
Tuberculosis screening at the Sainte-Anne Hospital in Paris - results of first and second IGRA.J Occup Med Toxicol. 2014 Jul 8;9:24. doi: 10.1186/1745-6673-9-24. eCollection 2014. J Occup Med Toxicol. 2014. PMID: 25018775 Free PMC article.
-
Serial IGRA testing of trainees in the healthcare sector in a country with low incidence for tuberculosis - a prospective cohort study.GMS Hyg Infect Control. 2013 Nov 6;8(2):Doc17. doi: 10.3205/dgkh000217. eCollection 2013. GMS Hyg Infect Control. 2013. PMID: 24327943 Free PMC article.
-
QFT-Plus: a plus in variability? - Evaluation of new generation IGRA in serial testing of students with a migration background in Germany.J Occup Med Toxicol. 2017 Jan 5;12:1. doi: 10.1186/s12995-016-0148-z. eCollection 2017. J Occup Med Toxicol. 2017. PMID: 28070206 Free PMC article.
-
Serial testing with the interferon-γ release assay in Portuguese healthcare workers.Int Arch Occup Environ Health. 2011 Apr;84(4):461-9. doi: 10.1007/s00420-010-0571-x. Epub 2010 Aug 19. Int Arch Occup Environ Health. 2011. PMID: 20721576 Free PMC article.
-
Serial testing for latent tuberculosis infection in transplant candidates: a retrospective review.Transpl Infect Dis. 2016 Feb;18(1):14-21. doi: 10.1111/tid.12489. Epub 2016 Feb 3. Transpl Infect Dis. 2016. PMID: 26671024 Review.
Cited by
-
Interferon-Gamma Release Assays versus Tuberculin Skin Testing for the Diagnosis of Latent Tuberculosis Infection: An Overview of the Evidence.Pulm Med. 2013;2013:601737. doi: 10.1155/2013/601737. Epub 2013 Feb 7. Pulm Med. 2013. PMID: 23476763 Free PMC article.
-
Tuberculosis screening at the Sainte-Anne Hospital in Paris - results of first and second IGRA.J Occup Med Toxicol. 2014 Jul 8;9:24. doi: 10.1186/1745-6673-9-24. eCollection 2014. J Occup Med Toxicol. 2014. PMID: 25018775 Free PMC article.
-
The effect of introducing IGRA to screen French healthcare workers for tuberculosis and potential conclusions for the work organisation.J Occup Med Toxicol. 2013 May 7;8:12. doi: 10.1186/1745-6673-8-12. eCollection 2013. J Occup Med Toxicol. 2013. PMID: 23647777 Free PMC article.
-
Interferon-gamma release assays for the tuberculosis serial testing of health care workers: a systematic review.J Occup Med Toxicol. 2012 Jun 18;7(1):6. doi: 10.1186/1745-6673-7-6. J Occup Med Toxicol. 2012. PMID: 22537915 Free PMC article.
-
Occupational screening for tuberculosis and the use of a borderline zone for interpretation of the IGRA in German healthcare workers.PLoS One. 2014 Dec 26;9(12):e115322. doi: 10.1371/journal.pone.0115322. eCollection 2014. PLoS One. 2014. PMID: 25541947 Free PMC article.
References
-
- Seidler A, Nienhaus A, Diel R. Review of epidemiological studies on the occupational risk of tuberculosis in low-incidence areas. Respiration. 2005;72(4):431–446. doi: 10.1159/000086261. Available from: http://dx.doi.org/10.1159/000086261. - DOI - DOI - PubMed
-
- Mazurek GH, Jereb J, Lobue P, Iademarco MF, Metchock B, Vernon A. Guidelines for using the QuantiFERON-TB Gold test for detecting Mycobacterium tuberculosis infection, United States. MMWR Recomm Rep. 2005;54(RR-15):49–55. - PubMed
-
- Deutsche Gesetzliche Unfallversicherung. Guidelines for Occupational Medical Examination - Prophylaxis in Occupational Medicine. 4 ed. Stuttgart: Gentner Verlag; 2007.
-
- Pai M, Dheda K, Cunningham J, Scano F, O'Brien R. T-cell assays for the diagnosis of latent tuberculosis infection: moving the research agenda forward. Lancet Infect Dis. 2007;7(6):428–438. doi: 10.1016/S1473-3099(07)70086-5. Available from: http://dx.doi.org/10.1016/S1473-3099(07)70086-5. - DOI - DOI - PubMed
LinkOut - more resources
Full Text Sources
