

Child abuse: the role of the orthopaedic surgeon in nonaccidental trauma
- PMID: 20941649
- PMCID: PMC3032840
- DOI: 10.1007/s11999-010-1610-3
Child abuse: the role of the orthopaedic surgeon in nonaccidental trauma
Abstract
Background: Child abuse presents in many different forms: physical, sexual, psychological, and neglect. The orthopaedic surgeon is involved mostly with physical abuse but should be aware of the other forms. There is limited training regarding child abuse, and the documentation is poor when a patient is at risk for abuse. There is a considerable risk to children when abuse is not recognized.
Questions/purposes: In this review, we (1) define abuse, (2) describe the incidence and demographic characteristics of abuse, (3) describe the orthopaedic manifestations of abuse, and (4) define the orthopaedic surgeon's role in cases of abuse.
Methods: We performed a PubMed literature review and a search of the Department of Health and Human Services Web site. The Pediatric Orthopaedic Surgery of North America trauma symposium was referenced and expanded to create this review.
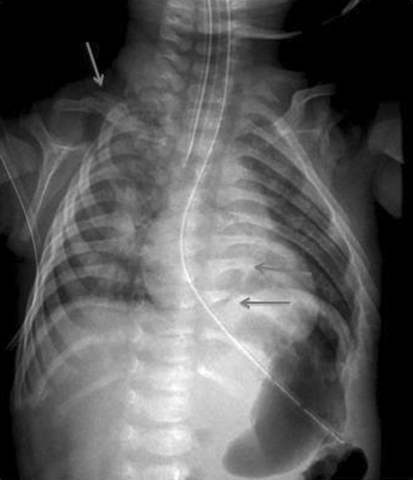
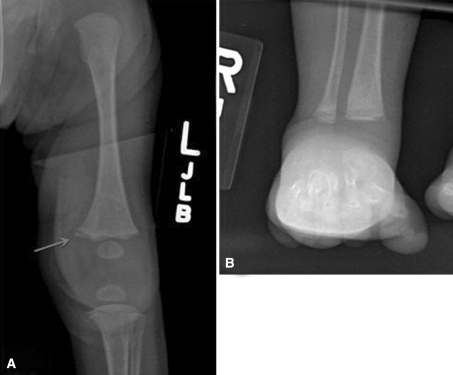
Results: Recognition and awareness of child abuse are the primary tasks of the orthopaedic surgeon. Skin trauma is more common than fractures, yet fractures are the most common radiographic finding. Patients with fractures who are younger than 3 years, particularly those younger than 1 year, should be evaluated for abuse. No fracture type or location is pathognomonic. Management in the majority of fracture cases resulting from abuse is nonoperative casting or splinting.
Conclusions: The role of the orthopaedic surgeon in suspected cases of child abuse includes (1) obtaining a good history and making a thorough physical examination; (2) obtaining the appropriate radiographs and notifying the appropriate services; and (3) participating in and communicating with a multidisciplinary team to manage the patients.
Figures
References
-
- Akbarnia BA, Akbarnia NO. The role of orthopedist in child abuse and neglect. Orthop Clin North Am. 1976;7:733–742. - PubMed
-
- Byrd SE, Harwood-Nash DC, Fitz CR, Barry JF, Rogovitz DM. Two projection computed tomography: the axial and Towne projections. Radiology. 1978;128:512–514. - PubMed
-
- Caffey J. Multiple fractures in the long bones of infants suffering from chronic subdural hematoma. AJR Am J Roentgenol. 1946;56:163–173. - PubMed
-
- Hinton RY, Lincoln A, Crockett MM, Sponsellor P, Smith G. Fractures of the femoral shaft in children: incidence, mechanisms, and sociodemographics risk factors. J Bone Joint Surg Am. 1999;81:500–509. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
