

Aging and sleep: physiology and pathophysiology
- PMID: 20941662
- PMCID: PMC3500384
- DOI: 10.1055/s-0030-1265902
Aging and sleep: physiology and pathophysiology
Abstract
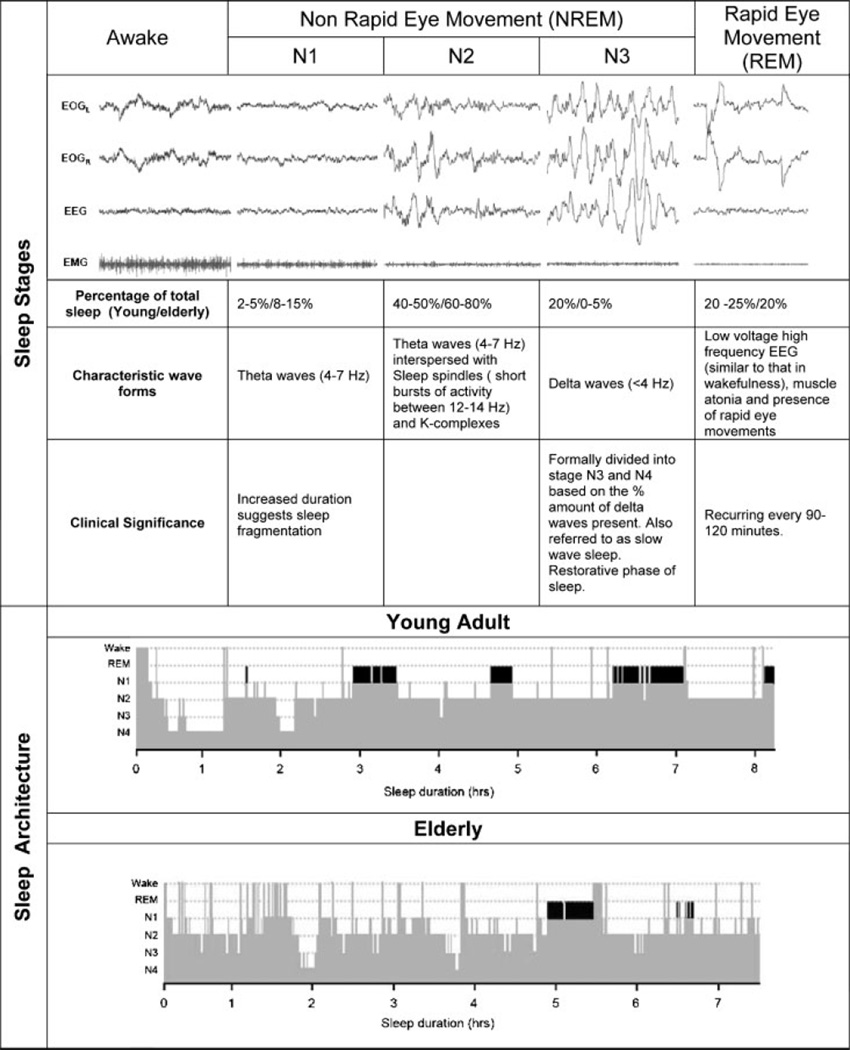
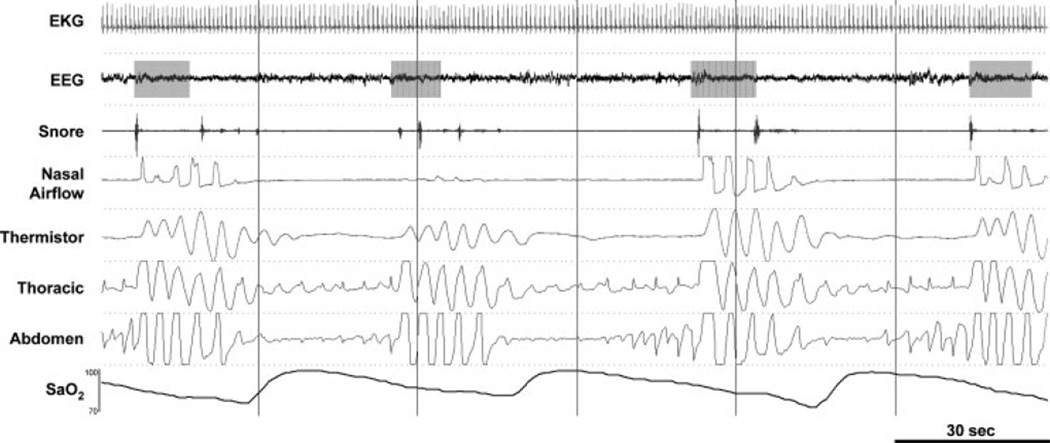
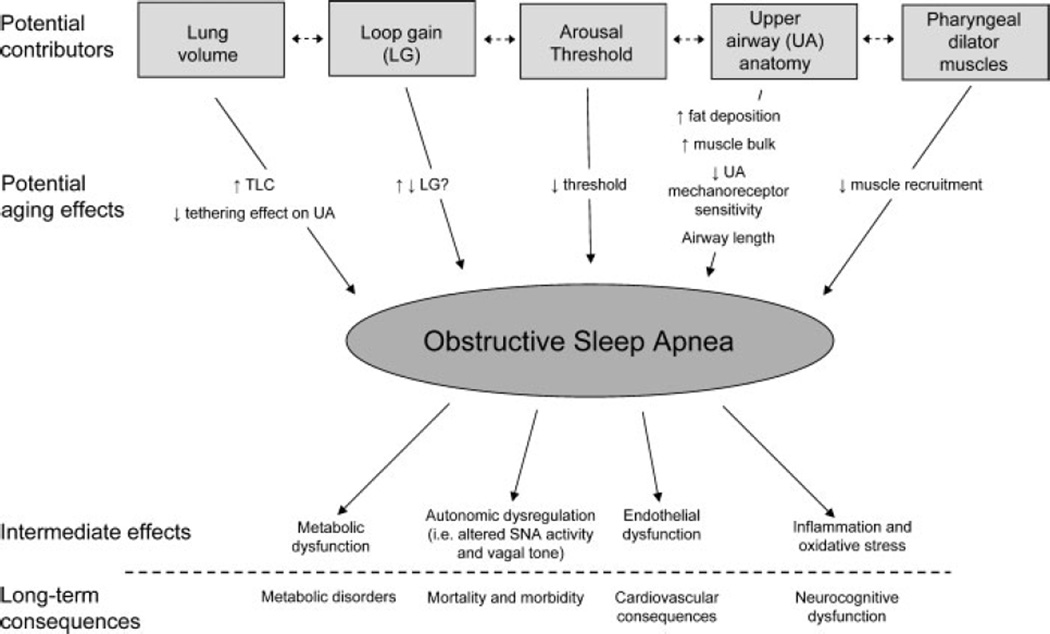
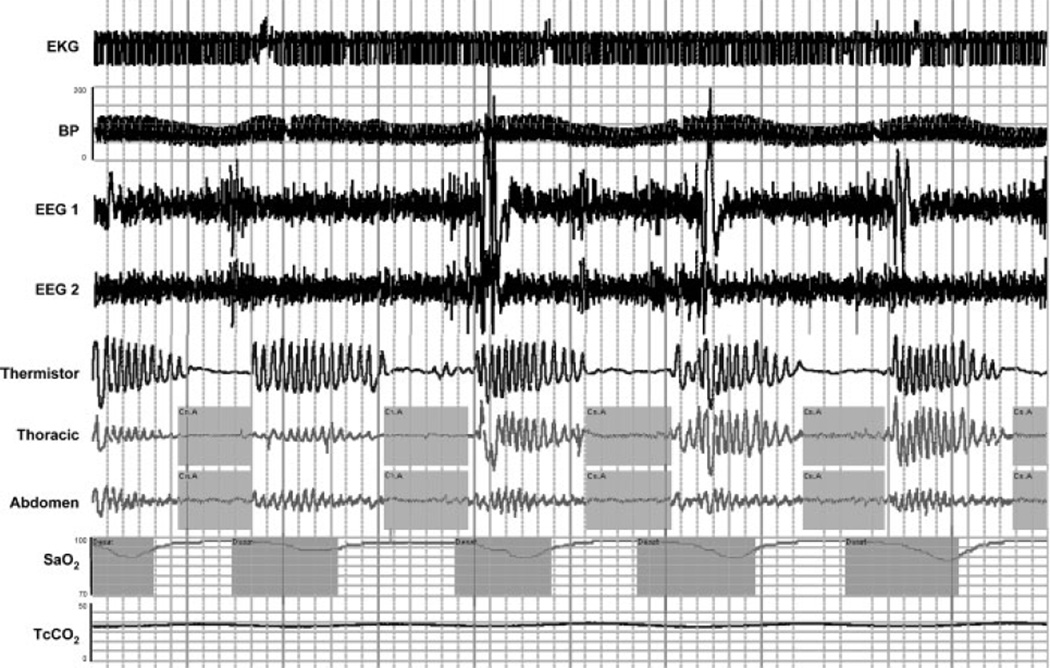
Aging effects on sleep are important to consider for the practicing pulmonologist due to the increase in prevalence of major respiratory disorders as well as the normal changes that occur in sleep patterns with aging. Typically, aging is associated with decreases in the amount of slow wave sleep and increases in stage 1 and 2 non-rapid eye movement sleep, often attributed to an increased number of spontaneous arousals that occur in the elderly. Elderly individuals tend to go to sleep earlier in the evening and wake earlier due to a phase advance in their normal circadian sleep cycle. Furthermore the development of sleep-related respiratory disorders such as obstructive sleep apnea (OSA) and central sleep apnea or Cheyne-Stokes respiration (CSA-CSR) associated with congestive heart failure (CHF) occur with increasing prevalence in the elderly. The development of such disorders is often of major concern because they are associated with systemic hypertension and cardiovascular disease, metabolic disorders such as diabetes, and impaired neurocognition. The present review reflects the current understanding of the normal changes in sleep patterns and sleep needs with advancing age, in addition to the effect that aging has on the predisposition to and consequences of OSA and CSA-CSR associated with CHF.
© Thieme Medical Publishers.
Figures
References
-
- Verstraeten E. Neurocognitive effects of obstructive sleep apnea syndrome. Curr Neurol Neurosci Rep. 2007;7:161–166. - PubMed
-
- Ferrara M, De Gennaro L, Casagrande M, Bertini M. Selective slow-wave sleep deprivation and time-of-night effects on cognitive performance upon awakening. Psychophysiology. 2000;37:440–446. - PubMed
-
- Weissman MM, Greenwald S, Niño-Murcia G, Dement WC. The morbidity of insomnia uncomplicated by psychiatric disorders. Gen Hosp Psychiatry. 1997;19:245–250. - PubMed
-
- Leproult R, Copinschi G, Buxton O, Van Cauter E. Sleep loss results in an elevation of cortisol levels the next evening. Sleep. 1997;20:865–870. - PubMed
-
- Scheen AJ, Byrne MM, Plat L, Leproult R, Van Cauter E. Relationships between sleep quality and glucose regulation in normal humans. Am J Physiol. 1996;271(2 Pt 1):E261–E270. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
