

Carotid plaque assessment using fast 3D isotropic resolution black-blood MRI
- PMID: 20941742
- PMCID: PMC3042490
- DOI: 10.1002/mrm.22642
Carotid plaque assessment using fast 3D isotropic resolution black-blood MRI
Abstract
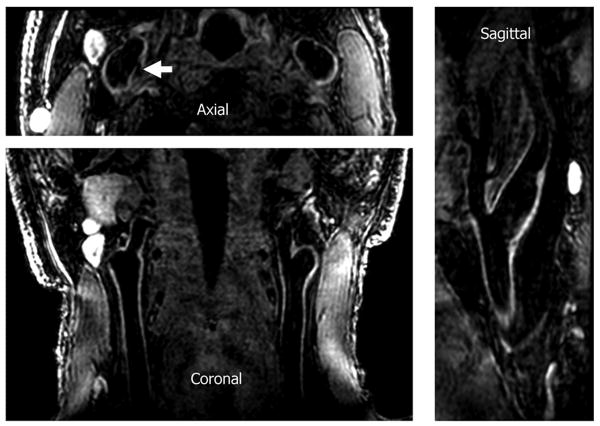
Black-blood MRI is a promising tool for carotid atherosclerotic plaque burden assessment and compositional analysis. However, current sequences are limited by large slice thickness. Accuracy of measurement can be improved by moving to isotropic imaging but can be challenging for patient compliance due to long scan times. We present a fast isotropic high spatial resolution (0.7×0.7×0.7 mm3) three-dimensional black-blood sequence (3D-MERGE) covering the entire cervical carotid arteries within 2 min thus ensuring patient compliance and diagnostic image quality. The sequence is optimized for vessel wall imaging of the carotid bifurcation based on its signal properties. The optimized sequence is validated on patients with significant carotid plaque. Quantitative plaque morphology measurements and signal-to-noise ratio measures show that 3D-MERGE provides good blood suppression and comparable plaque burden measurements to existing MRI protocols. 3D-MERGE is a promising new tool for fast and accurate plaque burden assessment in patients with atherosclerotic plaque.
Copyright © 2010 Wiley-Liss, Inc.
Figures










Similar articles
-
Three-Dimensional Carotid Plaque MR Imaging.Neuroimaging Clin N Am. 2016 Feb;26(1):1-12. doi: 10.1016/j.nic.2015.09.001. Epub 2015 Oct 19. Neuroimaging Clin N Am. 2016. PMID: 26610656 Free PMC article. Review.
-
Relaxation enhanced compressed sensing three-dimensional black-blood vessel wall MR imaging: Preliminary studies.Magn Reson Imaging. 2015 Sep;33(7):932-8. doi: 10.1016/j.mri.2015.03.009. Epub 2015 Apr 8. Magn Reson Imaging. 2015. PMID: 25863136
-
Turbo fast three-dimensional carotid artery black-blood MRI by combining three-dimensional MERGE sequence with compressed sensing.Magn Reson Med. 2013 Nov;70(5):1347-52. doi: 10.1002/mrm.24579. Epub 2012 Dec 27. Magn Reson Med. 2013. PMID: 23280949
-
Novel methodology for 3D reconstruction of carotid arteries and plaque characterization based upon magnetic resonance imaging carotid angiography data.Magn Reson Imaging. 2012 Oct;30(8):1068-82. doi: 10.1016/j.mri.2012.03.004. Epub 2012 May 21. Magn Reson Imaging. 2012. PMID: 22617149
-
Low-Grade Carotid Stenosis: Implications of MR Imaging.Neuroimaging Clin N Am. 2016 Feb;26(1):129-45. doi: 10.1016/j.nic.2015.09.010. Epub 2015 Oct 23. Neuroimaging Clin N Am. 2016. PMID: 26610665 Review.
Cited by
-
An objective method to optimize the MR sequence set for plaque classification in carotid vessel wall images using automated image segmentation.PLoS One. 2013 Oct 23;8(10):e78492. doi: 10.1371/journal.pone.0078492. eCollection 2013. PLoS One. 2013. PMID: 24194941 Free PMC article.
-
Three-Dimensional Carotid Plaque MR Imaging.Neuroimaging Clin N Am. 2016 Feb;26(1):1-12. doi: 10.1016/j.nic.2015.09.001. Epub 2015 Oct 19. Neuroimaging Clin N Am. 2016. PMID: 26610656 Free PMC article. Review.
-
Carotid artery atherosclerosis and white matter lesions in the elderly: a community-based MR imaging study.Eur Radiol. 2025 Sep;35(9):5561-5568. doi: 10.1007/s00330-025-11509-0. Epub 2025 Mar 20. Eur Radiol. 2025. PMID: 40108010
-
Imaging the carotid atherosclerotic plaque.Vasc Biol. 2019 Jun 28;1(1):H53-H58. doi: 10.1530/VB-19-0010. eCollection 2019. Vasc Biol. 2019. PMID: 32923954 Free PMC article. Review.
-
Efficient and Accurate 3D Thickness Measurement in Vessel Wall Imaging: Overcoming Limitations of 2D Approaches Using the Laplacian Method.J Cardiovasc Dev Dis. 2024 Aug 15;11(8):249. doi: 10.3390/jcdd11080249. J Cardiovasc Dev Dis. 2024. PMID: 39195157 Free PMC article.
References
-
- Fayad Z, Fuster V. Clinical imaging of the high-risk or vulnerable atherosclerotic plaque. Circ Res. 2001;89(4):305–316. - PubMed
-
- Yuan C, Kerwin WS. MRI of atherosclerosis. J Magn Reson Imaging. 2004;19(6):710–719. - PubMed
-
- Takaya N, Yuan C, Chu B, Saam T, Underhill H, Cai J, Tran N, Polissar N, Isaac C, Ferguson M, Garden G, Cramer S, Maravilla K, Hashimoto B, Hatsukami T. Association between carotid plaque characteristics and subsequent ischemic cerebrovascular events: a prospective assessment with MRI--initial results. Stroke. 2006;37(3):818–823. - PubMed
-
- Underhill H, Yuan C, Zhao X, Kraiss L, Parker D, Saam T, Chu B, Takaya N, Liu F, Polissar N, Neradilek B, Raichlen J, Cain V, Waterton J, Hamar W, Hatsukami T. Effect of rosuvastatin therapy on carotid plaque morphology and composition in moderately hypercholesterolemic patients: a high-resolution magnetic resonance imaging trial. Am Heart J. 2008;155(3):581–588. - PubMed
-
- Antiga L, Wasserman B, Steinman D. On the overestimation of early wall thickening at the carotid bulb by black blood MRI, with implications for coronary and vulnerable plaque imaging. Magn Reson Med. 2008;60(5):1020–1028. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
