

CA125 immune complexes in ovarian cancer patients with low CA125 concentrations
- PMID: 20943848
- PMCID: PMC3079311
- DOI: 10.1373/clinchem.2010.153122
CA125 immune complexes in ovarian cancer patients with low CA125 concentrations
Abstract
Background: About 20% of women with ovarian cancer have low concentrations of serum cancer antigen 125 (CA125), and this important tumor marker cannot be used to monitor their disease. The measured concentration for mucin 1 (MUC1), or CA15-3, another tumor marker, can be lowered in breast and ovarian cancer patients when circulating immune complexes (CICs) containing antibodies bound to the free antigen are present. Because CA125 and MUC1 are related members of the mucin family, we sought to determine whether CICs might also exist for CA125 and interfere with its clinical assay.
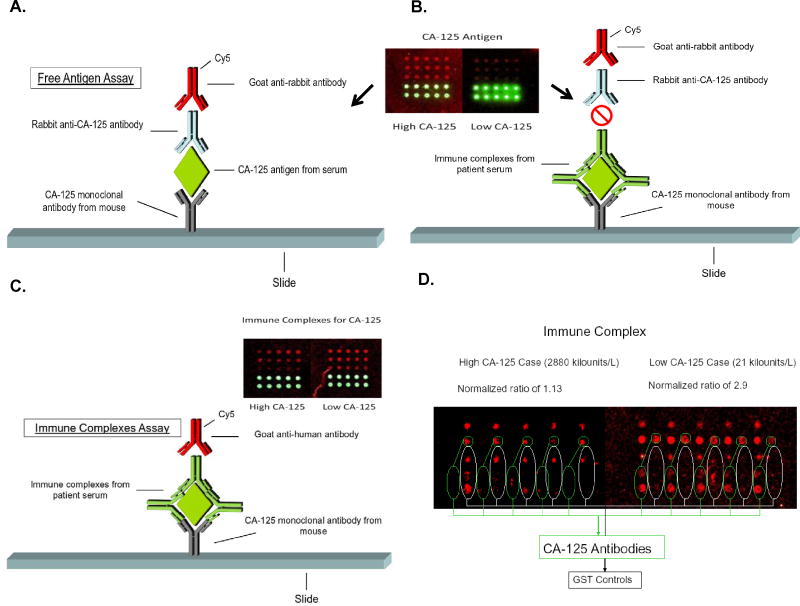
Methods: We developed an antigen capture-based assay to determine the presence of CICs for CA125. We spotted mouse antibodies to CA125 onto nanoparticle slides, incubated them with patient serum, and added Cy5-tagged goat antihuman IgG antibodies. Fluorescence intensities were read and normalized to the intensities for glutathione S-transferase A1 as a control.
Results: Assay results for 23 ovarian cancer cases with high CA125 concentrations, 43 cases with low CA125 concentrations, and 19 controls (mean CA125 concentrations, 2706, 23, and 11 kilounits/L, respectively) revealed mean fluorescence intensities for CA125 CIC of 2.30, 2.72, and 1.99 intensity units (iu), respectively. A generalized linear model adjusted for batch and age showed higher CA125 CIC fluorescence intensities in low-CA125 cases than in high-CA125 cases (P = 0.03) and controls (P = 0.0005). Four ovarian cancer patients who had recurrent disease and always had low CA125 values had a mean CA125 CIC value of 3.06 iu (95% CI, 2.34-4.01 iu).
Conclusions: These preliminary results suggest the existence of CICs involving CA125, which may help explain some ovarian cancer cases with low CA125 concentrations.
Conflict of interest statement
Figures
References
-
- Bast RC, Jr, Klug TL, St John E, Jenison E, Niloff JM, Lazarus H, et al. A radioimmunoassay using a monoclonal antibody to monitor the course of epithelial ovarian cancer. N Engl J Med. 1983;309:883–7. - PubMed
-
- Yin BW, Lloyd KO. Molecular cloning of the CA125 ovarian cancer antigen: identification as a new mucin, MUC16. J Biol Chem. 2001;276:27371–5. - PubMed
-
- Cooper BC, Sood AK, Davis CS, Ritchie JM, Sorosky JI, Anderson B, Buller RE. Preoperative CA 125 levels: an independent prognostic factor for epithelial ovarian cancer. Obstet Gynecol. 2002;100:59–64. - PubMed
-
- Geisler JP, Miller GA, Lee TH, Harwood RM, Wiemann MC, Geisler HE. Relationship of preoperative serum CA-125 to survival in epithelial ovarian carcinoma. J Reprod Med. 1996;41:140–2. - PubMed
-
- Buller RE, Berman ML, Bloss JD, Manetta A, DiSaia PJ. Serum CA125 regression in epithelial ovarian cancer: correlation with reassessment findings and survival. Gynecol Oncol. 1992;47:87–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
