

An update on idiopathic intracranial hypertension
- PMID: 20944524
- PMCID: PMC3674489
An update on idiopathic intracranial hypertension
Abstract
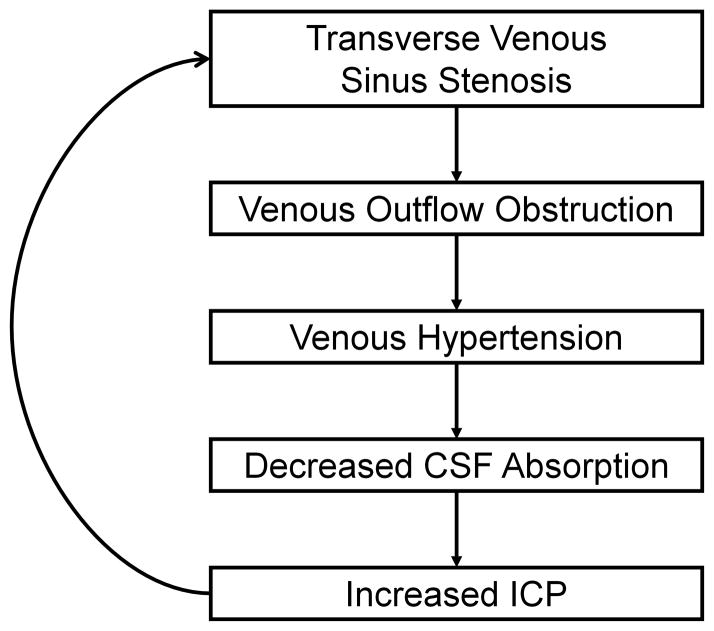
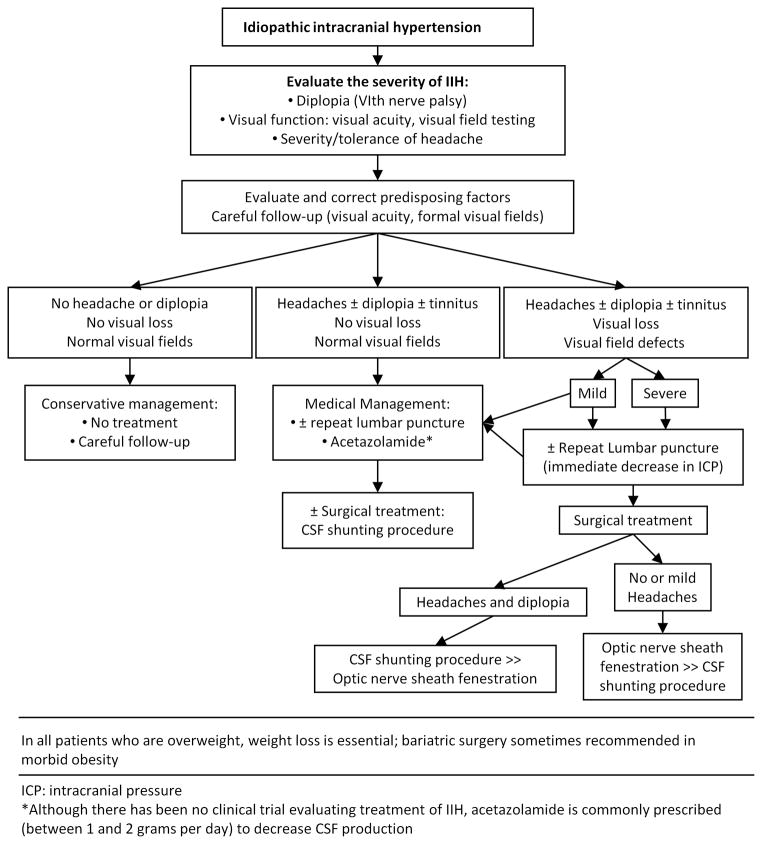
Idiopathic intracranial hypertension (IIH) is a condition of unknown etiology often encountered in neurologic practice. It produces nonlocalizing symptoms and signs of raised intracranial pressure and, when left untreated, can result in severe irreversible visual loss. It most commonly occurs in obese women of childbearing age, but it can also occur in children, men, nonobese adults, and older adults. Although it is frequently associated with obesity, it can be associated with other conditions, such as obstructive sleep apnea and transverse cerebral venous sinus stenoses. Recent identification of subgroups at high risk for irreversible visual loss, including black patients, men, and patients with fulminant forms of IIH, help guide the optimal management and follow-up. Ongoing studies of venous anatomy and physiology in IIH patients, as well as a recently begun randomized clinical treatment trial, should provide further insight into this common yet poorly understood syndrome.
Figures
References
-
- Friedman DI, Jacobson DM. Diagnostic criteria for idiopathic intracranial hypertension. Neurology. 2002;59:1492–1495. - PubMed
-
- Biousse V, Ameri A, Bousser MG. Isolated intracranial hypertension as the only sign of cerebral venous thrombosis. Neurology. 1999;53:1537–1542. - PubMed
-
- Digre KB, Corbett JJ. Idiopathic intracranial hypertension (pseudotumor cerebri): a reappraisal. Neurologist. 2001;7:2–67.
-
- Friedman DI, Jacobson DM. Idiopathic intracranial hypertension. J Neuroophthalmol. 2004;24:138–145. - PubMed
-
- Digre KB. Three current controversies in idiopathic intracranial hypertension. Neuroophthalmology. 2009;33:93–99.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical