

Changing epidemiology of trauma deaths leads to a bimodal distribution
- PMID: 20944754
- PMCID: PMC2943446
- DOI: 10.1080/08998280.2010.11928649
Changing epidemiology of trauma deaths leads to a bimodal distribution
Abstract
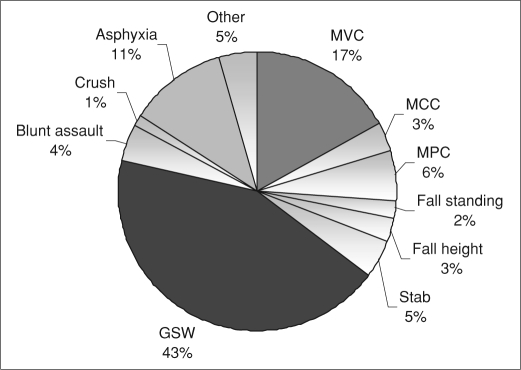
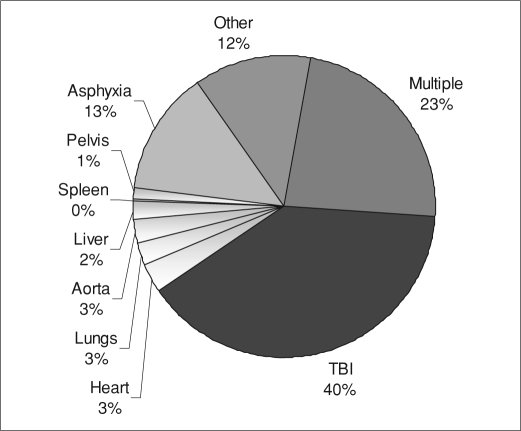
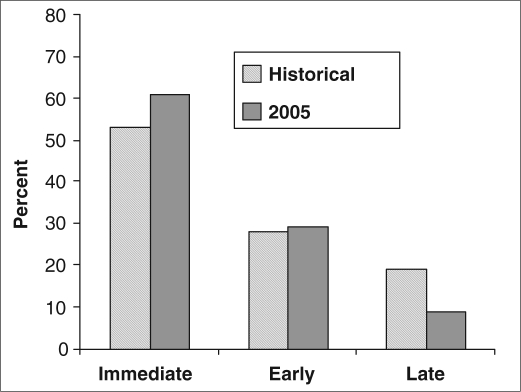
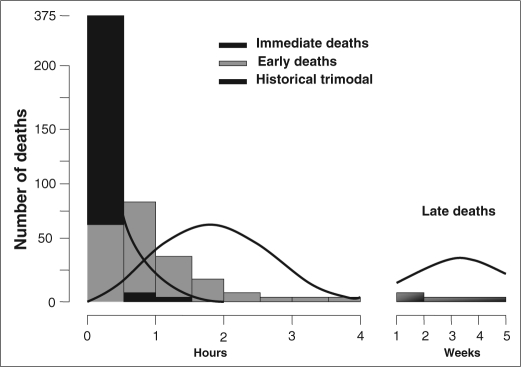
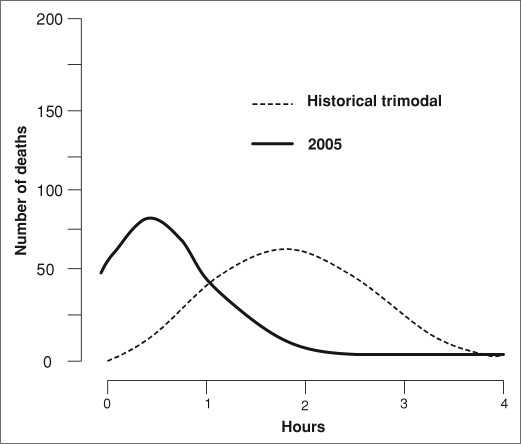
Injury mortality was classically described with a trimodal distribution, with immediate deaths at the scene, early deaths due to hemorrhage, and late deaths from organ failure. We hypothesized that the development of trauma systems has improved prehospital care, early resuscitation, and critical care and altered this pattern. This population-based study of all trauma deaths in an urban county with a mature trauma system reviewed data for 678 patients (median age, 33 years; 81% male; 43% gunshot, 20% motor vehicle crashes). Deaths were classified as immediate (scene), early (in hospital, ≤4 hours from injury), or late (>4 hours after injury). Multinomial regression was used to identify independent predictors of immediate and early versus late deaths, adjusted for age, gender, race, intention, mechanism, toxicology, and cause of death. Results showed 416 (61%) immediate, 199 (29%) early, and 63 (10%) late deaths. Compared with the classical description, the percentage of immediate deaths remained unchanged, and early deaths occurred much earlier (median 52 vs 120 minutes). However, unlike the classic trimodal distribution, the late peak was greatly diminished. Intentional injuries, alcohol intoxication, asphyxia, and injuries to the head and chest were independent predictors of immediate death. Alcohol intoxication and injuries to the chest were predictors of early death, while pelvic fractures and blunt assaults were associated with late deaths. In conclusion, trauma deaths now have a predominantly bimodal distribution. Near elimination of the late peak likely represents advancements in resuscitation and critical care that have reduced organ failure. Further reductions in mortality will likely come from prevention of intentional injuries and injuries associated with alcohol intoxication.
Figures
References
-
- Cowley RA. The resuscitation and stabilization of major multiple trauma patients in a trauma center environment. Clin Med. 1976;83:16–22.
-
- Cowley RA. A total emergency medical system for the state of Maryland. Md State Med J. 1975;24(7):37–45. - PubMed
-
- Trunkey DD. Trauma. Sci Am. 1983;249:28–35. - PubMed
-
- West JG, Trunkey DD, Lim RC. Systems of trauma care. A case of two counties. Arch Surg. 1979;114(4):455–460. - PubMed
-
- Meislin H, Criss EA, Judkins D, Berger R, Conroy C, Parks B, Spaite DW, Valenzuela TD. Fatal trauma: the modal distribution of time to death is a function of patient demographics and regional resources. J Trauma. 1997;43(3):433–440. - PubMed
LinkOut - more resources
Full Text Sources