

Local, regional, and systemic recurrence rates in patients undergoing skin-sparing mastectomy compared with conventional mastectomy
- PMID: 20945319
- PMCID: PMC4371507
- DOI: 10.1002/cncr.25505
Local, regional, and systemic recurrence rates in patients undergoing skin-sparing mastectomy compared with conventional mastectomy
Abstract
Background: Although the use of SSM is becoming more common, there are few data on long-term, local-regional, and distant recurrence rates after treatment. The purpose of this study was to examine the rates of local, regional, and systemic recurrence, and survival in breast cancer patients who underwent skin-sparing mastectomy (SSM) or conventional mastectomy (CM) at our institution.
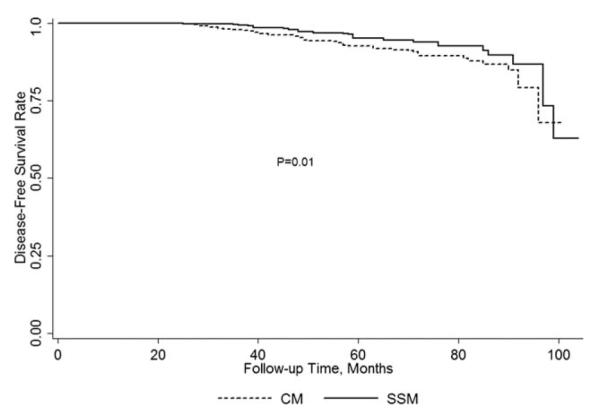
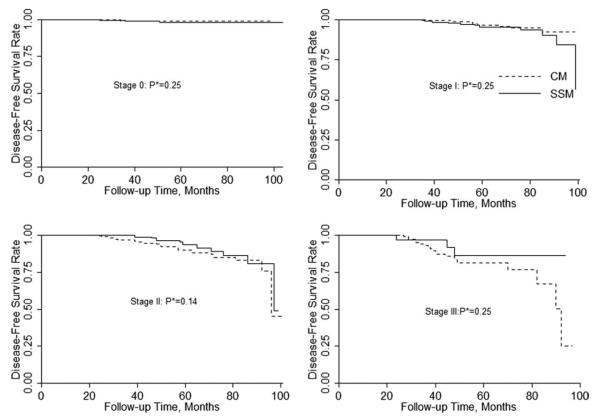
Methods: Patients with stage 0 to III unilateral breast cancer who underwent total mastectomy at our center from 2000 to 2005 were included in this study. Kaplan-Meier curves were calculated, and the log-rank test was used to evaluate the differences between overall and disease-free survival rates in the 2 groups.
Results: Of 1810 patients, 799 (44.1%) underwent SSM and 1011 (55.9%) underwent CM. Patients who underwent CM were older (58.3 vs 49.3 years, P<.0001) and were more likely to have stage IIB or III disease (53.0% vs 31.8%, P<.0001). Significantly more patients in the CM group received neoadjuvant chemotherapy and adjuvant radiation therapy (P<.0001). At a median follow-up of 53 months, 119 patients (6.6%) had local, regional, or systemic recurrences. The local, regional, and systemic recurrence rates did not differ significantly between the SSM and CM groups. After adjusting for clinical TNM stage and age, disease-free survival rates between the SSM and CM groups did not differ significantly.
Conclusions: SSM is an acceptable treatment option for patients who are candidates for immediate breast reconstruction. Local-regional recurrence rates are similar to those of patients undergoing CM. Cancer 2011. © 2010 American Cancer Society.
Copyright © 2010 American Cancer Society.
Figures

Similar articles
-
Long-term Oncologic Outcomes of Immediate Breast Reconstruction vs Conventional Mastectomy Alone for Breast Cancer in the Setting of Neoadjuvant Chemotherapy.JAMA Surg. 2020 Dec 1;155(12):1142-1150. doi: 10.1001/jamasurg.2020.4132. JAMA Surg. 2020. PMID: 33052412 Free PMC article.
-
Nipple skin-sparing mastectomy is feasible for advanced disease.Ann Surg Oncol. 2013 Oct;20(10):3294-302. doi: 10.1245/s10434-013-3174-4. Epub 2013 Aug 22. Ann Surg Oncol. 2013. PMID: 23975304
-
Prediction of margin involvement and local recurrence after skin-sparing and simple mastectomy.Eur J Surg Oncol. 2016 Jul;42(7):935-41. doi: 10.1016/j.ejso.2016.04.055. Epub 2016 May 3. Eur J Surg Oncol. 2016. PMID: 27256869
-
Recurrence of breast carcinoma following immediate reconstruction: a 13-year review.Plast Reconstr Surg. 1994 Jan;93(1):96-106; discussion 107-8. Plast Reconstr Surg. 1994. PMID: 8278489 Review.
-
Patterns of invasive recurrence among patients originally treated for ductal carcinoma in situ by breast-conserving surgery versus mastectomy.Breast Cancer Res Treat. 2021 Apr;186(3):617-624. doi: 10.1007/s10549-021-06129-3. Epub 2021 Mar 6. Breast Cancer Res Treat. 2021. PMID: 33675490 Free PMC article. Review.
Cited by
-
The Utility of Indocyanine Green Angiography in Breast Reconstruction to Detect Mastectomy Skin Flap Necrosis and Free Flap Perfusion: An Umbrella Review.Bioengineering (Basel). 2024 Oct 15;11(10):1025. doi: 10.3390/bioengineering11101025. Bioengineering (Basel). 2024. PMID: 39451401 Free PMC article. Review.
-
Robotic nipple-sparing mastectomy for the treatment of breast cancer: Feasibility and safety study.Breast. 2017 Feb;31:51-56. doi: 10.1016/j.breast.2016.10.009. Epub 2016 Nov 2. Breast. 2017. PMID: 27810700 Free PMC article.
-
The Usefulness of Magnetic Resonance Imaging (MRI) for the Detection of Local Recurrence after Mastectomy with Reconstructive Surgery in Breast Cancer Patients.Diagnostics (Basel). 2022 Sep 11;12(9):2203. doi: 10.3390/diagnostics12092203. Diagnostics (Basel). 2022. PMID: 36140604 Free PMC article.
-
Comparison of Local Recurrence After Simple and Skin-Sparing Mastectomy Performed in Patients with Ductal Carcinoma In Situ.Ann Surg Oncol. 2017 Apr;24(4):1071-1076. doi: 10.1245/s10434-016-5673-6. Epub 2016 Nov 11. Ann Surg Oncol. 2017. PMID: 27837296 Free PMC article.
-
Oncological safety of nipple-sparing mastectomy in young patients with breast cancer compared with conventional mastectomy.Oncol Lett. 2018 Apr;15(4):4813-4820. doi: 10.3892/ol.2018.7913. Epub 2018 Jan 31. Oncol Lett. 2018. PMID: 29541245 Free PMC article.
References
-
- Freeman BS. Subcutaneous mastectomy for benign breast lesions with immediate or delayed prosthetic replacement. Plast Reconstr Surg Transplant Bull. 1962;30:676–682. - PubMed
-
- Toth BA, Lappert P. Modified skin incisions for mastectomy: the need for plastic surgical input in preoperative planning. Plast Reconstr Surg. 1991;87:1048–1053. - PubMed
-
- Carlson GW, Styblo TM, Lyles RH, et al. The use of skin sparing mastectomy in the treatment of breast cancer: The Emory experience. Surg Oncol. 2003;12:265–269. - PubMed
-
- Foster RD, Esserman LJ, Anthony JP, et al. Skin-sparing mastectomy and immediate breast reconstruction: a prospective cohort study for the treatment of advanced stages of breast carcinoma. Ann Surg Oncol. 2002;9:462–466. - PubMed
-
- Garwood ER, Moore D, Ewing C, et al. Total skin-sparing mastectomy: complications and local recurrence rates in 2 cohorts of patients. Ann Surg. 2009;249:26–32. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
