

Trends of rheumatoid arthritis monitorization in Romania
- PMID: 20945825
- PMCID: PMC3019003
Trends of rheumatoid arthritis monitorization in Romania
Abstract
Background: rheumatoid arthritis (RA) is associated with the loss of overall functionality, which leads to substantial economic losses. Second line agents used in RA treatment require careful monitorization in terms of efficiency and tolerability.
Objective: trends, predictive factors and characteristics of clinical, biological and radiological RA monitorization in a cross sectional observational cohort study, conducted on over 206 patients in Romania, with a 12 months follow up (December 2007 - December 2008).
Method: Cases were recruited from the south-west region of the country, covering a geographical area of 23 counties. Patients were invited to complete three sets of interviews (collected by post) in a consent letter, containing self reported questionnaires, at 6 months intervals: an original questionnaire (which included quantitative self reported of pain, disease activity and fatigue on visual analogue scale-VAS), Health Assessment Questionnaire-HAQ-Disability and Discomfort Scales and EUROQOL EQ-5D, validated in Romanian (obtaining a user agreement by authors of the original version).
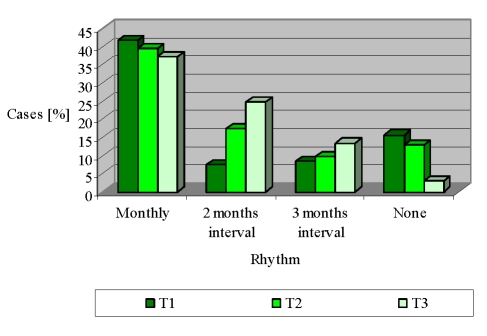
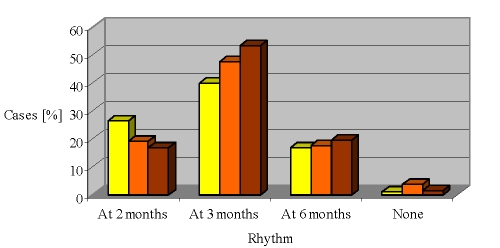
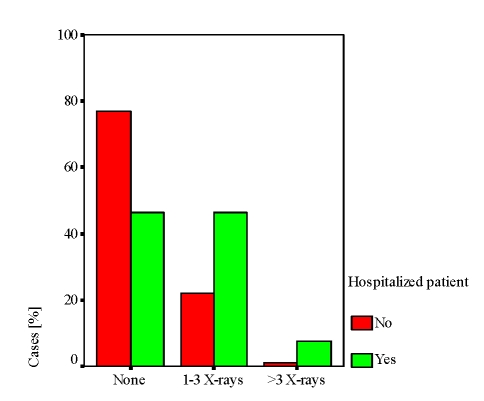
Results: analysis was carried out in SPSS 10. The cohort enrolled 206 patients, with the average age of 54.90 +/- 12.67 years, 66% urban, 86.4% women, 29.1% professionally active, 48.5% graduates of primary education. The average disease duration after diagnosis of RA was of 9.40 +/- 8.87 years. The duration of the treatment reported at baseline was of 2.70 +/- 2.64 years. Most patients followed a program of monthly monitoring at a general practitioner (GP) (41.7% at baseline and 37.1% to 12 months). Visits to the rheumatologist followed a monthly regimen (32.3% at baseline and 31.7% to 12 months) or a 2 months interval (19.4% at baseline and 29.6% to 12 months, p = 0.000). Biological monitoring was quarterly (39.6% and 53.2% at 12 months; p = 0.000) or at 2 months interval (26.2% at baseline and 16.7% to 12 months, p = 0.000). X-ray monitoring lacked in over half the cases in a year of disease progression (63.3% at 6 months and 62.2% at 12 months), although it sums between 1 and 3 radiographs to one third of the cases (36.8%),
Conclusion: generally, in our country, there is a lack of aggregation in the dispensarization algorithm of patients with RA; consequently, the decision is awarded to the human factor. Under these circumstances, some patients are over evaluated. Promoting a dispensarization guide for RA patients could induce benefits both clinically and economically. Therefore, we submit a proposal of recommendations as a guideline for clinical, biological and radiological monitoring, according to the phase and stage of RA.
Figures





References
-
- Breedveld F, Weisman M, Kavanaugh A. The PREMIER study: A multicenter, randomized, double–blind clinical trial of combination therapy with adalimumab plus methotrexate versus methotrexate alone or adalimumab alone in patients with early, aggressive rheumatoid arthritis who had not had previous methotrexate treatment. Arthritis and Rheumatism. 2006;54(1):26–37. - PubMed
-
- Chan G, Goh F, Hodgson T, Hsu S. Outpatient follow–up for patients with rheumatoid arthritis in relation to New Zealand Rheumatology Association guidelines at Dunedin Hospital . Journal of new Zealand Medical Association. 2008;121(1274) - PubMed
-
- Fernandez I, Varela C, Layola M, Ruiz MD, Navarro F. Using HAQ to estimate HUI3 and EQ–5D Utility values in Spanish Rheumatoid Arthritis Patients . ISPOR 11th Annual European Congress. 2008.
-
- Grassi W, De Angelis R, Lamanna G, Cervini C. The clinical features of rheumatoid arthritis . Eur J Radiol. 1998;27(8):18–24. - PubMed
-
- Guidelines for the Management of Rheumatoid Arthritis American College of Rheumatology Subcommittee on Rheumatoid Arthritis Guidelines. Arthritis and Rheumatism . 2002;46(2):328–346. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical