

Effects of edaravone on muscle atrophy and locomotor function in patients with ischemic stroke: a randomized controlled pilot study
- PMID: 20945946
- PMCID: PMC3585769
- DOI: 10.2165/11586550-000000000-00000
Effects of edaravone on muscle atrophy and locomotor function in patients with ischemic stroke: a randomized controlled pilot study
Erratum in
- Drugs R D. 2010;10(4):285
Abstract
Background and objective: Stroke patients with severe leg paralysis are often bedridden in the acute and subacute phase, which increases the risk of disuse muscle atrophy in the chronic phase. The evidence to date indicates that oxidative stress plays an important role in the mechanism of disuse muscle atrophy. Therefore, the aim of this study was to determine if long-term radical scavenger treatment with edaravone following an acute stroke prevents the progression of disuse muscle atrophy and improves leg locomotor function in the chronic phase.
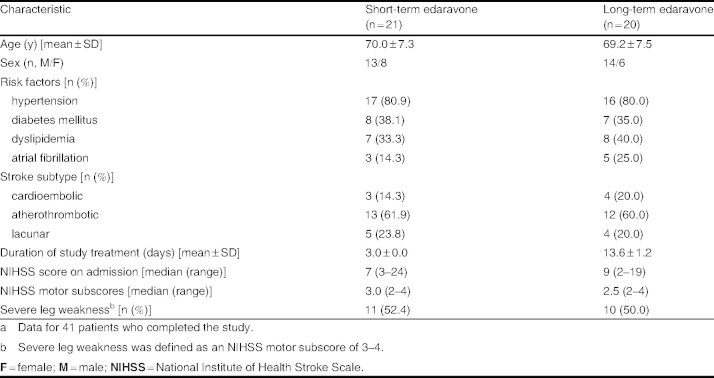
Methods: This randomized controlled pilot study was conducted at 19 acute stroke and rehabilitation centers across Japan. Forty-seven ischemic stroke patients with at least leg motor weakness admitted within 24 hours of onset were randomly assigned to receive continuous intravenous infusions of edaravone 30 mg twice daily for 3 days (short-term group) or 10-14 days (long-term group). The primary endpoints of the study included the degree of leg disuse muscle atrophy, as measured by the percentage change from baseline in femoral muscle circumference 15 cm above the knee, and the improvement in leg locomotor function, as assessed by the maximum walking speed over 10 m, 3 months after the onset of stroke.
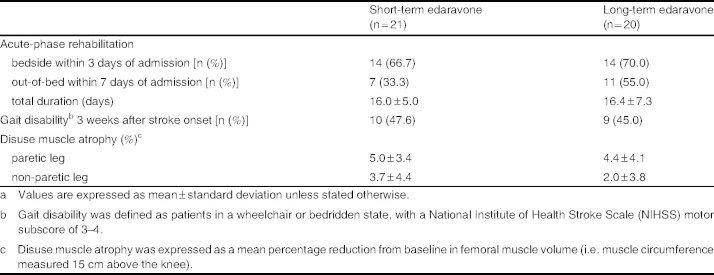
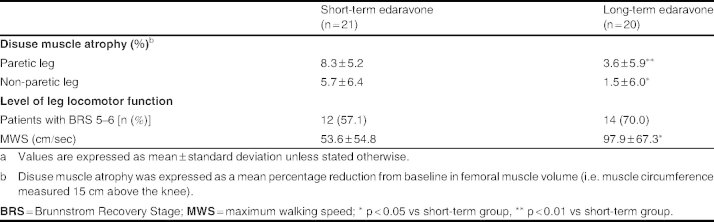
Results: Three-month follow-up was completed by a total of 41 patients (21 in the short-term group and 20 in the long-term group). On admission, there was no significant difference in the severity of stroke or the grade of leg paresis between the two treatment groups. The grade of disuse muscle atrophy and incidence of gait impairment 3 weeks after stroke onset were also similar between the short- and long-term groups. However, disuse muscle atrophy of the paretic and non-paretic legs was significantly less severe in the long-term versus the short-term treatment group (3.6 ± 5.9% and 1.5 ± 6.0% vs 8.3 ± 5.2% and 5.7 ± 6.4%; p < 0.01 and p < 0.05) 3 months after stroke onset. Additionally, the maximum walking speed over a distance of 10 m was significantly greater in the long-term group (98 ± 67 vs 54 ± 55 cm/sec; p < 0.05).
Conclusion: Edaravone treatment for up to 14 days suppresses the progression of disuse muscle atrophy and improves leg locomotor function to a greater extent than shorter-term treatment in acute stroke patients. This suggests that the management of stroke may be improved with long-term edaravone therapy by providing myoprotective effects that ameliorate functional outcome in the chronic phase.
Figures

References
-
- Kortebein P, Ferrando A, Lombeida J, et al. Effect of 10 days of bed rest on skeletal muscle in healthy older adults. JAMA. 2007;297(16):1772–4. - PubMed
-
- Kondo K, Ota T. Changes with time in cross-sectional areas of leg muscles in early stroke rehabilitation patients: disuse muscle atrophy and its recovery. Jpn J Rehabil Med. 1997;34:124–33.
-
- Odajima N, Ishiai S, Okiyama R, et al. CT findings of leg muscles in the hemiplegics due to cerebrovascular accidents: correlation to disuse atrophy. Rinsho Shinkeigaku. 1987;27(9):1154–62. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical