

Changing trends in intestinal parasitic infections among long-term-residents and settled immigrants in Qatar
- PMID: 20946623
- PMCID: PMC2972266
- DOI: 10.1186/1756-3305-3-98
Changing trends in intestinal parasitic infections among long-term-residents and settled immigrants in Qatar
Abstract
Background: The rapid socio-economic development in Qatar in the last two decades has encouraged a mass influx of immigrant workers, the majority of whom originate from countries with low socio-economic levels, inadequate medical care and many are known to carry patent intestinal helminth and protozoan infections on arrival in Qatar. Some eventually acquire residency status but little is known about whether they continue to harbour infections.
Methods: We examined 9208 hospital records of stool samples that had been analysed for the presence of intestinal helminth and protozoan ova/cysts, over the period 2005-2008, of subjects from 28 nationalities, but resident in Qatar and therefore not recent arrivals in the country.
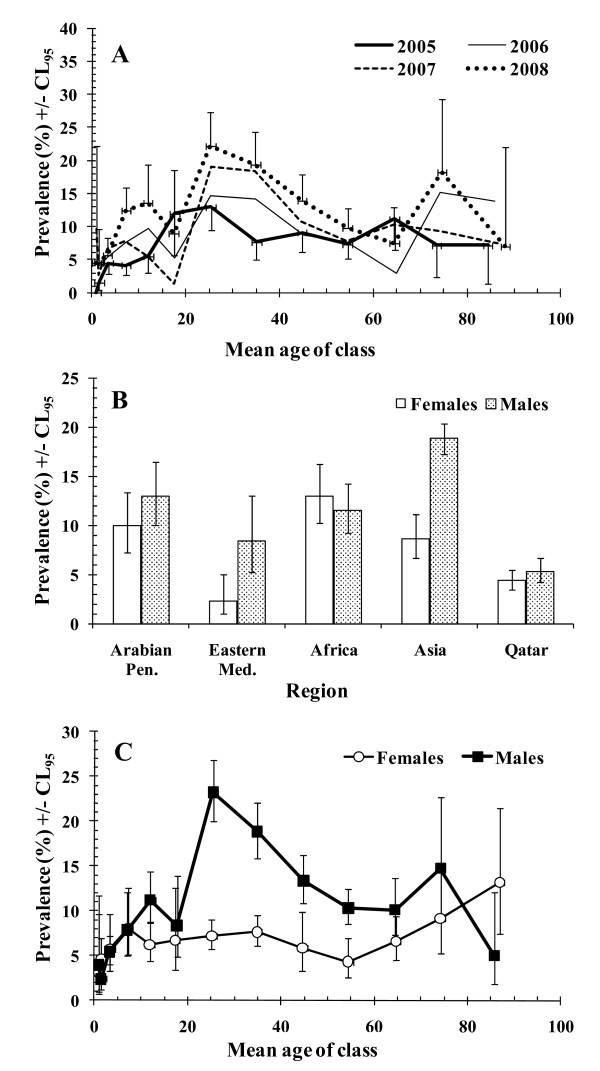
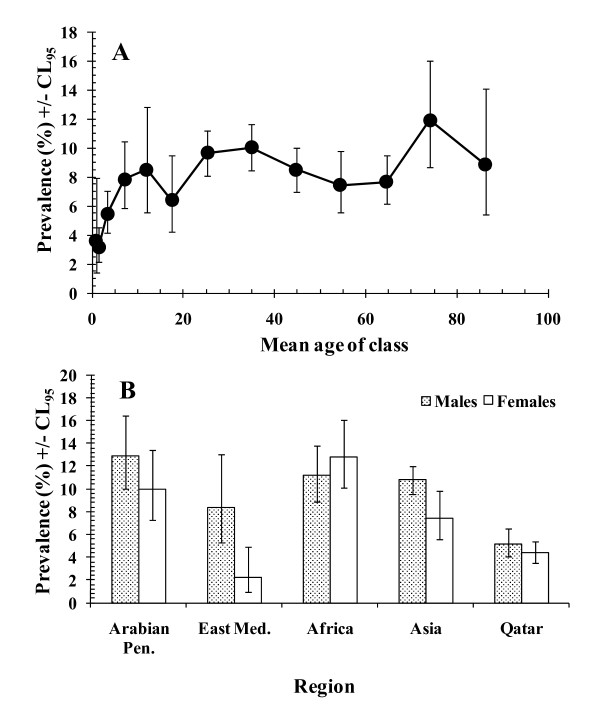
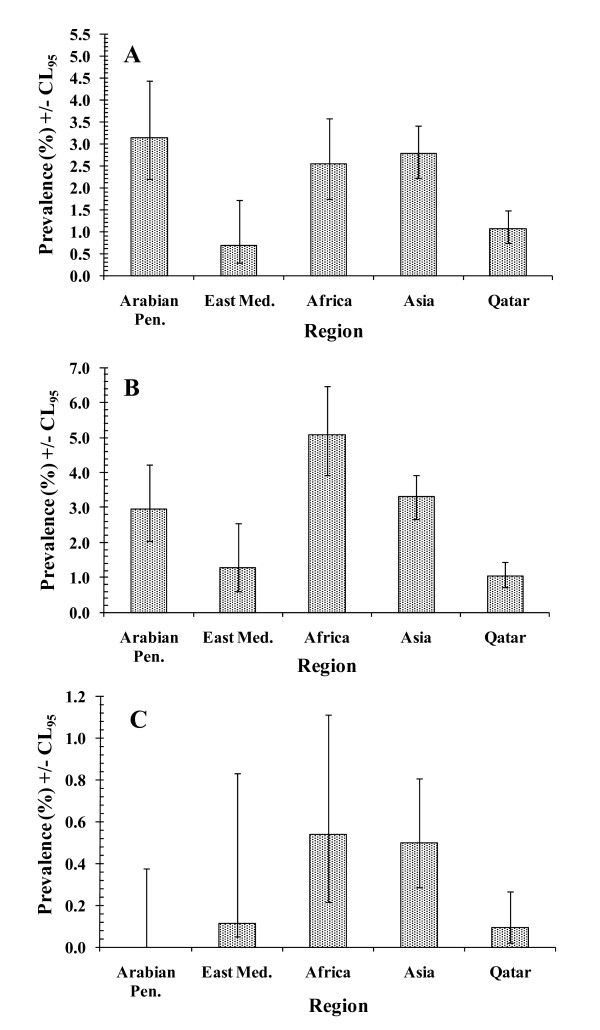
Results: Overall 10.2% of subjects were infected with at least one species, 2.6% with helminths and 8.0% with protozoan species. Although hookworms, Ascaris lumbricoides, Trichuris trichiura and Hymenolepis nana were observed, the majority of helminth infections (69%) were caused by hookworms, and these were largely aggregated among 20.0-39.9 year-old male subjects from Nepal. The remaining cases of helminth infection were mostly among Asian immigrants. Protozoan infections were more uniformly spread across immigrants from different regions when prevalence was calculated on combined data, but this disguised three quite contrasting underlying patterns for 3 taxa of intestinal protozoa. Blastocystis hominis, Giardia duodenalis and non-pathogenic amoebae were all acquired in childhood, but whereas prevalence of B. hominis rose to a plateau and then even further among the elderly, prevalence of G. duodenalis fell markedly in children aged 10 and older, and stayed low (< 2%) gradually falling even further in the elderly. In contrast the prevalence of non-pathogenic amoebae (Entamoeba coli, E. hartmanni, Endolimax nana and Iodamoeba buetschlii) peaked in the 30.0-39.9 age group and only then dropped to very low values among the oldest subjects examined. A worrying trend in respect of both helminth and protozoan parasites was the increase in prevalence over the period 2005-2008, in helminth infections prevalence increasing 2-3 fold by 2008, and in protozoan infections by 1.5-2.0 fold.
Conclusions: We suggest that helminth infections are probably acquired abroad when immigrants visit their home villages, whilst protozoan infections are reinforced by transmission in Qatar, possibly in the poorer areas of the state where immigrant workers live. We discuss the significance of these findings and emphasize that they have clear implications for the health authorities.
Figures

References
-
- Ibrahim OMG, Bener A, Shalabi A. Prevalence of intestinal parasites among expatriate workers in Al-Ain, United Arab Emirates. Ann Saudi Med. 1993;13:126–129. - PubMed
-
- Al-Madani AA, Mahfouz AA. Prevalence of intestinal parasitic infections among Asian female house keepers in Abha District, Saudi Arabia. S E Asian J Trop Med Pub Health. 1995;26:135–137. - PubMed
-
- Alkarmi T, Alharbi S, Abu-Lisan M, Salman A, Behbehani K. Prevalence of intestinal parasitic infections in Kuwait. Med Principles Pract. 1991;2:10–17.
LinkOut - more resources
Full Text Sources
