

Optical mapping of the isolated coronary-perfused human sinus node
- PMID: 20946995
- PMCID: PMC3008584
- DOI: 10.1016/j.jacc.2010.03.098
Optical mapping of the isolated coronary-perfused human sinus node
Abstract
Objectives: We sought to confirm our hypothesis that the human sinoatrial node (SAN) is functionally insulated from the surrounding atrial myocardium except for several exit pathways that electrically bridge the nodal tissue and atrial myocardium.
Background: The site of origin and pattern of excitation within the human SAN has not been directly mapped.
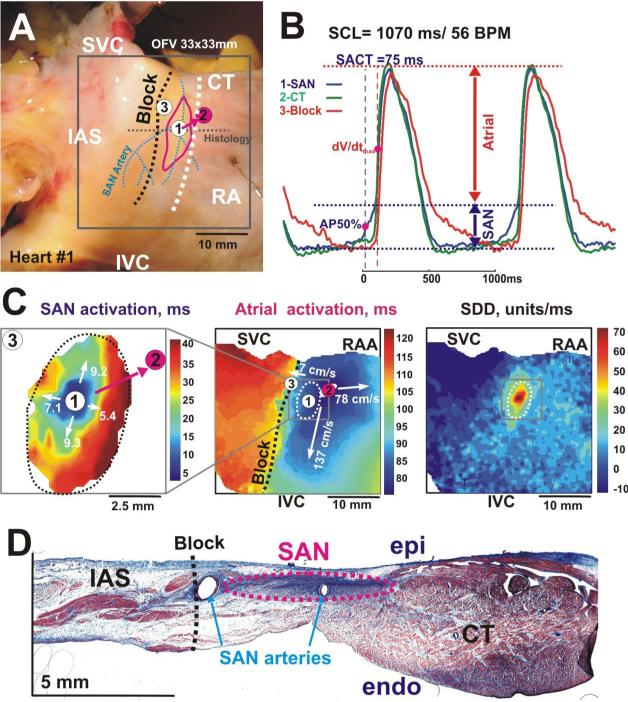
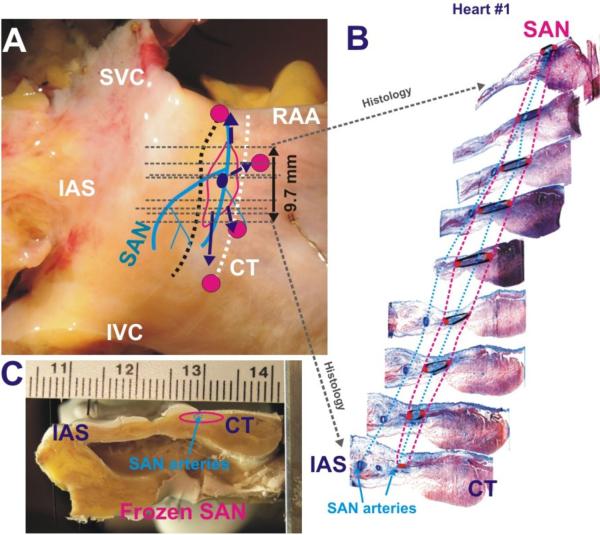
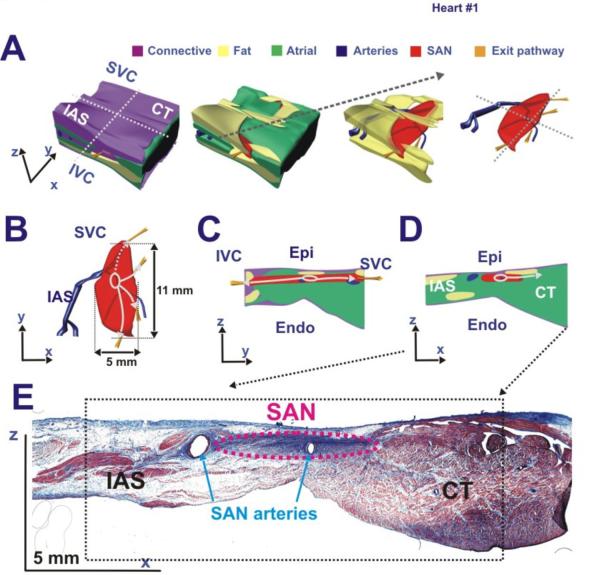
Methods: The SAN was optically mapped in coronary-perfused preparations from nonfailing human hearts (n = 4, age 54 ± 15 years) using the dye Di-4-ANBDQBS and blebbistatin. The SAN 3-dimensional structure was reconstructed using histology.
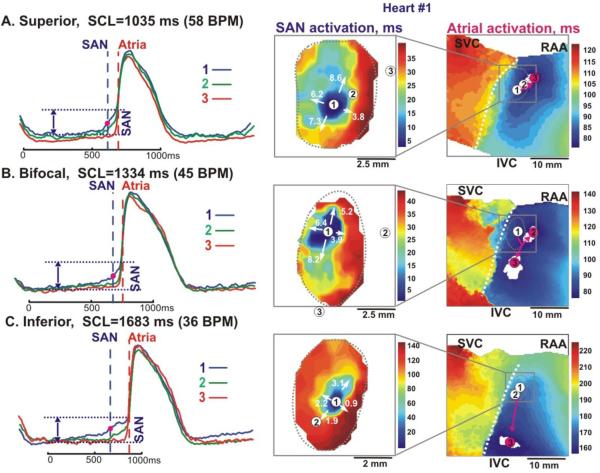
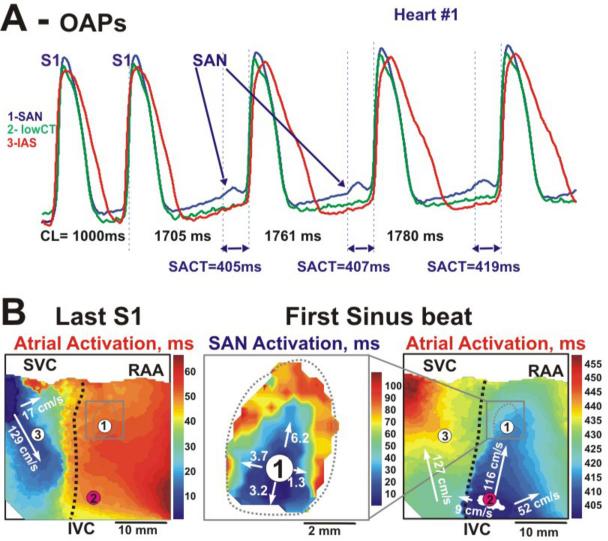
Results: Optical recordings from the SAN had diastolic depolarization and multiple upstroke components, which corresponded to the separate excitations of the SAN and atrial layers. Excitation originated in the middle of the SAN (66 ± 17 beats/min), and then spread slowly (1 to 18 cm/s) and anisotropically. After a 82 ± 17 ms conduction delay within the SAN, the atrial myocardium was excited via superior, middle, and/or inferior sinoatrial conduction pathways. Atrial excitation was initiated 9.4 ± 4.2 mm from the leading pacemaker site. The oval 14.3 ± 1.5 mm × 6.7 ± 1.6 mm × 1.0 ± 0.2 mm SAN structure was functionally insulated from the atrium by connective tissue, fat, and coronary arteries, except for these pathways.
Conclusions: These data demonstrated for the first time, to our knowledge, the location of the leading SAN pacemaker site, the pattern of excitation within the human SAN, and the conduction pathways into the right atrium. The existence of these pathways explains why, even during normal sinus rhythm, atrial breakthroughs could arise from a region parallel to the crista terminalis that is significantly larger (26.1 ± 7.9 mm) than the area of the anatomically defined SAN.
Copyright © 2010 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The tell-tale heart (now, optically mapped).J Am Coll Cardiol. 2010 Oct 19;56(17):1395-6. doi: 10.1016/j.jacc.2010.05.042. J Am Coll Cardiol. 2010. PMID: 20946996 No abstract available.
References
-
- Boyett MR, Honjo H, Kodama I. The sinoatrial node, a heterogeneous pacemaker structure. Cardiovasc Res. 2000;47:658–687. - PubMed
-
- Opthof T, de Jonge B, Jongsma HJ, et al. Functional morphology of the mammalian sinuatrial node. Eur Heart J. 1987;8:1249–1259. - PubMed
-
- Verkerk AO, van Ginneken AC, Wilders R. Pacemaker activity of the human sinoatrial node: role of the hyperpolarization-activated current, I(f) Int J Cardiol. 2009;132:318–336. - PubMed
-
- Schuessler RB. Abnormal sinus node function in clinical arrhythmias. J Cardiovasc Electrophysiol. 2003;14:215–217. - PubMed
-
- Bromberg BI, Hand DE, Schuessler RB, et al. Primary negativity does not predict dominant pacemaker location: implications for sinoatrial conduction. Am J Physiol. 1995;269:H877–H887. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
