

Prognostic value of global MR myocardial perfusion imaging in women with suspected myocardial ischemia and no obstructive coronary disease: results from the NHLBI-sponsored WISE (Women's Ischemia Syndrome Evaluation) study
- PMID: 20947048
- PMCID: PMC3278772
- DOI: 10.1016/j.jcmg.2010.07.008
Prognostic value of global MR myocardial perfusion imaging in women with suspected myocardial ischemia and no obstructive coronary disease: results from the NHLBI-sponsored WISE (Women's Ischemia Syndrome Evaluation) study
Abstract
Objectives: The purpose of this study was to assess the prognostic value of global magnetic resonance (MR) myocardial perfusion imaging (MPI) in women with suspected myocardial ischemia and no obstructive (stenosis <50%) coronary artery disease (CAD).
Background: The prognostic value of global MR-MPI in women without obstructive CAD remains unknown.
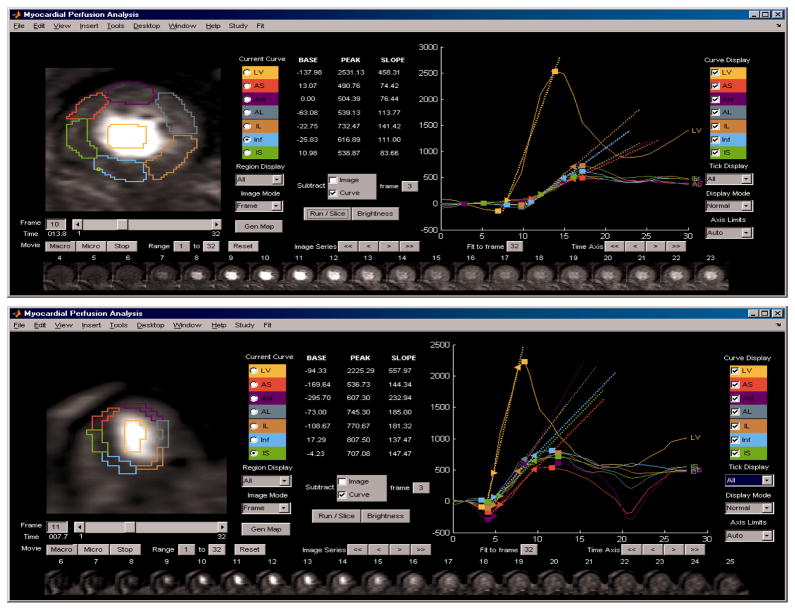
Methods: Women (n = 100, mean age 57 ± 11 years, age range 31 to 76 years), with symptoms of myocardial ischemia and with no obstructive CAD, as assessed by coronary angiography, underwent MR-MPI and standard functional assessment. During follow-up (34 ± 16 months), time to first adverse event (death, myocardial infarction, or hospitalization for worsening anginal symptoms) was analyzed using global MPI and left ventricular ejection fraction (EF) data.
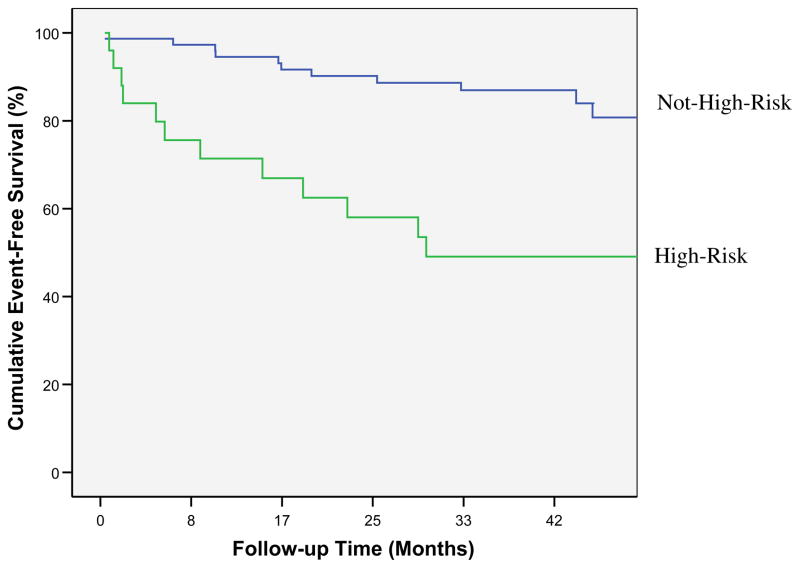
Results: Adverse events occurred in 23 (23%) women. Using univariable Cox proportional hazards regression modeling, variables found to be predictive of adverse events were global MR-MPI average uptake slope (p < 0.05), the ratio of MR-MPI peak signal amplitude to uptake slope (p < 0.05), and EF (p < 0.05). Two multivariable Cox models were formed, 1 using variables that were performance site dependent: ratio of MR-MPI peak amplitude to uptake slope together with EF (chi square: 13, p < 0.005); and a model using variables that were performance site independent: MR-MPI slope and EF (chi square: 12, p < 0.005). Each of the 2 multivariable models remained predictive of adverse events after adjustment for age, disease history, and Framingham risk score. For each of the Cox models, patients were categorized as high risk if they were in the upper quartile of the model and as not high risk otherwise. Kaplan-Meier analysis of time to event was performed for high risk versus not high risk for site-dependent (log rank: 15.2, p < 0.001) and site-independent (log rank: 13.0, p < 001) models.
Conclusions: Among women with suspected myocardial ischemia and no obstructive CAD, MR-MPI-determined global measurements of normalized uptake slope and peak signal uptake, together with global functional assessment of EF, appear to predict prognosis.
Copyright © 2010 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Mieres JH, Shaw LJ, Arai A, Budoff MJ, et al. Cardiac Imaging Committee. Role of Noninvasive Testing in the Clinical Evaluation of Women With Suspected Coronary Artery Disease Consensus Statement From the Cardiac Imaging Committee, Council on Clinical Cardiology, and the Cardiovascular Imaging and Intervention Committee, Council on Cardiovascular Radiology and Intervention, American Heart Association. Circulation. 2005;111:682–696. - PubMed
-
- Vaccarino V, Parsons L, Every NR, Barron HV, Krumholz HM. Sex-based differences in early mortality after myocardial infarction. National Registry of Myocardial Infarction 2 Participants. New England J Med. 1999;341(4):217–25. - PubMed
-
- Benjamin EJ, Smith SC, Jr, Cooper RS, Hill MN, Luepker RV. Task force #1--magnitude of the prevention problem: opportunities and challenges. 33rd Bethesda Conference. J Am Coll Cardiol. 2002;40(4):588–603. - PubMed
-
- Gordon EE. Coronary artery disease in women: the role of diagnostic imaging. Echocardiography. 1993;10(3):321–30. - PubMed
-
- Shaw LJ, Hachamovitch R, Redberg RF. Current evidence on diagnostic testing in women with suspected coronary artery disease: choosing the appropriate test. Cardiol in Rev. 2000;8(1):65–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
