

The quality of pain management in German hospitals
- PMID: 20948774
- PMCID: PMC2947845
- DOI: 10.3238/arztebl.2010.0607
The quality of pain management in German hospitals
Abstract
Background: The Pain-Free Hospital Project was initiated in 2003 with the aim of improving pain management throughout Germany. We assessed the current state of pain management in German hospitals.
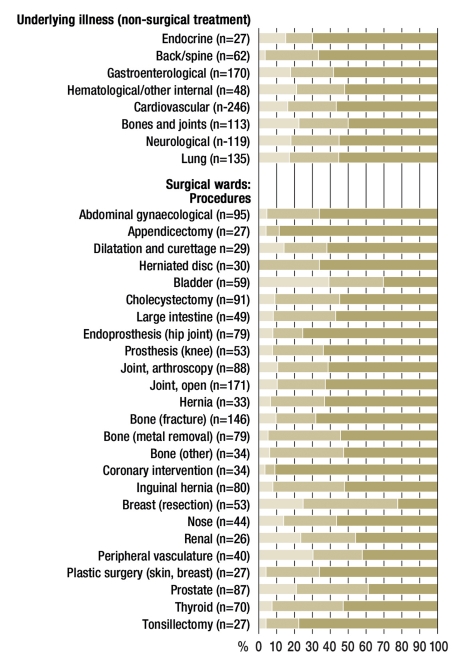
Methods: From 2004 to 2006, data were obtained anonymously from 2252 patients who had undergone surgery, and 999 who had been treated non-surgically, in a total of 25 hospitals. They were interviewed about the intensity of pain they had experienced and about the effectiveness of its treatment.
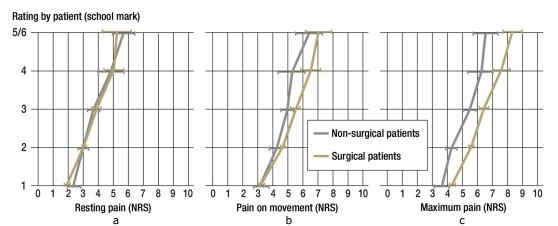
Results: No pain at all was reported by 12.4% of patients who had undergone surgery and by 16.7% of the non-surgically treated patients. Moderate to severe pain at rest was reported by 29.5% of the surgical group and 36.8% of the non-surgical group. More than 50% of the overall group reported pain on movement. 55% of the surgical group, and 57% of the non-surgical group, were dissatisfied with their pain management. Peak pain tended to occur outside normal working hours. No analgesic treatment at all was given to 39% of patients in the non-surgical group, even though they were in pain; the corresponding figure for the surgical group was 15% (a significant difference, p<0.001). Inadequately effective pain management was reported by 45.6% of patients in the non-surgical group and 29.6% in the operative group (again, a significant difference. Cancer patients were treated more often with potent opioids.
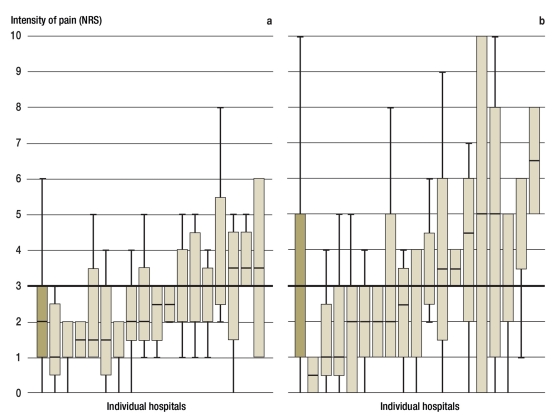
Conclusion: Severe postoperative pain is still too common among hospitalized patients, particularly pain that is induced by movement. Patients being treated on non-surgical wards also often suffer severe pain needlessly. Pain management seems to be worse for non-surgical patients (cancer patients excepted) than for surgical patients: waiting times for medication are longer, and ineffective medications are given more often. On the other hand, a number of hospitals provide positive examples of the potential effectiveness of pain management for both surgical and non-surgical patients.
Figures
Comment in
-
Unacceptable pain.Dtsch Arztebl Int. 2010 Nov;107(47):844. doi: 10.3238/arztebl.2010.0844. Epub 2010 Nov 26. Dtsch Arztebl Int. 2010. PMID: 21173906 Free PMC article. No abstract available.
References
-
- Jage J, Tryba M, Neugebauer E, et al. Postoperative Schmerztherapie - eine interdisziplinäre Notwendigkeit. Dtsch Arztebl. 2005;102(6)
-
- AWMF. S3-Leitlinie: Behandlung akuter perioperativer und post-traumatischer Schmerzen. www.uni-duesseldorf.de/AWMF/ll/041-001.htm
-
- Block BM, Liu SS, Rowlingson AJ, Cowan AR, Cowan JA, Jr, Wu CL. Efficacy of postoperative epidural analgesia: a meta-analysis. JAMA. 2003;290:2455–2463. - PubMed
-
- Brodner G, Mertes N, Buerkle H, Marcus MA, Van Aken H. Acute pain management: analysis, implications and consequences after prospective experience with 6349 surgical patients. Eur J Anaesth. 2000;17:566–575. - PubMed
-
- de Leon-Casasola O, Lema MJ, Karabella D, Harrison P. Epidural analgesia versus intravenous patient-controlled analgesia: Differences in the postoperative course of cancer patients. Reg Anesth. 1994;19:307–315. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical