

Five-year long-term outcomes of laparoscopic surgery for colon cancer
- PMID: 20954288
- PMCID: PMC2957610
- DOI: 10.3748/wjg.v16.i39.4992
Five-year long-term outcomes of laparoscopic surgery for colon cancer
Abstract
Aim: To perform a meta-analysis to answer whether long-term recurrence rates after laparoscopic-assisted surgery are comparable to those reported after open surgery.
Methods: A comprehensive literature search of the MEDLINE database, EMBASE database, and the Cochrane Central Register of Controlled Trials for the years 1991-2010 was performed. Prospective randomized clinical trials (RCTs) were eligible if they included patients with colon cancer treated by laparoscopic surgery vs open surgery and followed for more than five years.
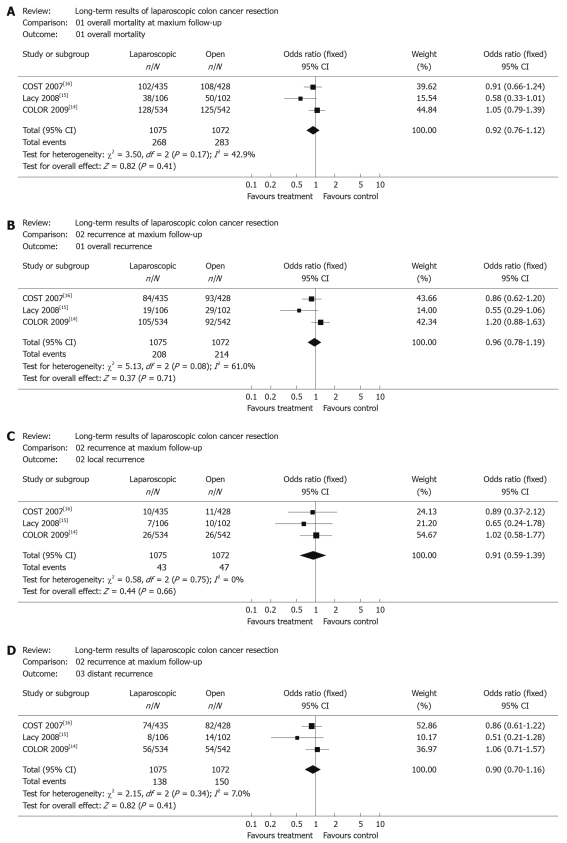
Results: Three studies involving 2147 patients reported long-term outcomes based on five-year data and were included in the analysis. The overall mortality was similar in the two groups (24.9%, 268/1075 in the laparoscopic group and 26.4%, 283/1072 in open group). No significant differences between laparoscopic and open surgery were found in overall mortality during the follow-up period of these studies [OR (fixed) 0.92, 95% confidence intervals (95% CI): 0.76-1.12, P = 0.41]. No significant difference in the development of overall recurrence was found in colon cancer patients, when comparing laparoscopic and open surgery [2147 pts, 19.3% vs 20.0%; OR (fixed) 0.96, 95% CI: 0.78-1.19, P = 0.71].
Conclusion: This meta-analysis suggests that laparoscopic surgery was as efficacious and safe as open surgery for colon cancer, based on the five-year data of these included RCTs.
Figures
References
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Barkun JS, Barkun AN, Sampalis JS, Fried G, Taylor B, Wexler MJ, Goresky CA, Meakins JL. Randomised controlled trial of laparoscopic versus mini cholecystectomy. The McGill Gallstone Treatment Group. Lancet. 1992;340:1116–1119. - PubMed
-
- Cooperman AM, Katz V, Zimmon D, Botero G. Laparoscopic colon resection: a case report. J Laparoendosc Surg. 1991;1:221–224. - PubMed
-
- Jacobs M, Verdeja JC, Goldstein HS. Minimally invasive colon resection (laparoscopic colectomy) Surg Laparosc Endosc. 1991;1:144–150. - PubMed
-
- Lacy AM, García-Valdecasas JC, Delgado S, Castells A, Taurá P, Piqué JM, Visa J. Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet. 2002;359:2224–2229. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
