

The challenge of mixed cerebrovascular disease
- PMID: 20955421
- PMCID: PMC4364441
- DOI: 10.1111/j.1749-6632.2010.05758.x
The challenge of mixed cerebrovascular disease
Abstract
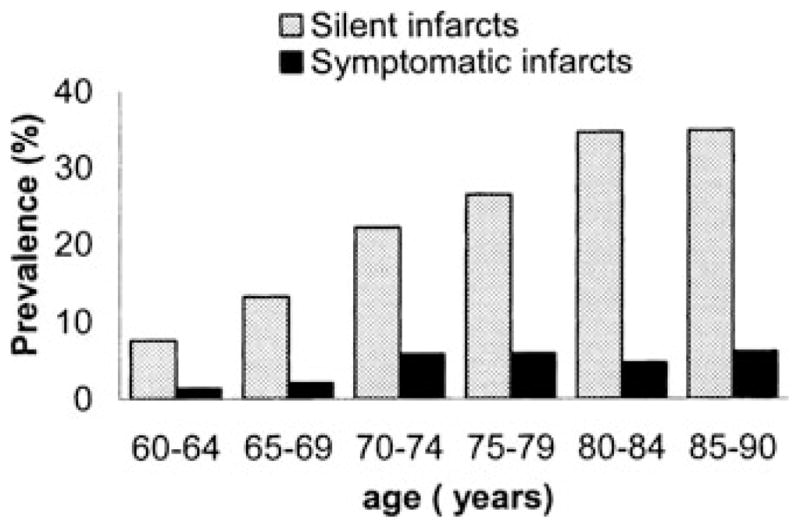
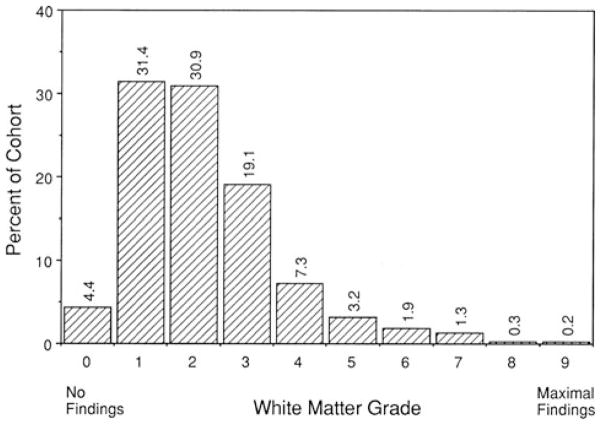
Stroke in general, and ischemic stroke in particular, are routinely defined using clinical criteria. Incorporating brain imaging and neuropathological findings into an expanded conceptual definition of stroke will result in a vastly increased prevalence of the disease. The resultant category of mixed cerebrovascular disease thus may include subclinical infarct, cerebral white matter disease, and cerebral microbleeds. Subclinical brain infarcts occur five times more frequently than does clinical ischemic stroke. Abnormalities of cerebral white matter are present in more than 95% of the population over the age of 65 years, and magnetic resonance imaging evidence of cerebral microbleeds is found in at least 18% of the population, beginning at the age of 60 years. Pathologic evidence supports at least a partial microvascular origin for cerebral white matter disease and cerebral microbleeds. Emphasizing mixed cerebrovascular disease as a conceptual framework allows for a focus on common underlying mechanisms and new therapeutic strategies.
© 2010 New York Academy of Sciences.
Conflict of interest statement
Boehringer–Ingelheim: research grant, speakers’ bureau, and honoraria; Otsuka Pharmaceutical Co.: research grant and honoraria.
Figures
References
-
- Easton JD, Saver JL, Albers GW, et al. Definition and evaluation of transient ischemic attack. Stroke. 2009;40:2276–2293. - PubMed
-
- Lloyd-Jones D, Adams RJ, Brown TM, et al. Heart disease and stroke statistics-2010 update: a report from the American Heart Association. Circulation. 2010;121:e46–e215. - PubMed
-
- Vermeer SE, Koudstaal PJ, Oudkerek M, et al. Prevalence and risk factors of silent brain infarcts in the population-based Rotterdam scan study. Stroke. 2002;33:21–25. - PubMed
-
- Pantoni L, Basile AM, Pracucci G, et al. Impact of age-related cerebral white matter changes on the transition to disability–the LADIS study: rationale, design, and methodology. Neuroepidemiology. 2005;24:51–62. - PubMed
-
- Longstreth WT, Manolio TA, Arnold A, et al. Clinical correlates of white matter findings on cranial magnetic resonance imaging of 3301 elderly people. Stroke. 1996;27:1274–1282. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
