

Quantitative upright-supine high-speed SPECT myocardial perfusion imaging for detection of coronary artery disease: correlation with invasive coronary angiography
- PMID: 20956478
- PMCID: PMC3130607
- DOI: 10.2967/jnumed.110.078782
Quantitative upright-supine high-speed SPECT myocardial perfusion imaging for detection of coronary artery disease: correlation with invasive coronary angiography
Abstract
A recently developed camera system for high-speed SPECT (HS-SPECT) myocardial perfusion imaging shows excellent correlation with conventional SPECT. Our goal was to test the diagnostic accuracy of an automated quantification of combined upright and supine myocardial SPECT for detection of coronary artery disease (CAD) (≥ 70% luminal diameter stenosis or, in left main coronary artery, ≥ 50% luminal diameter stenosis) in comparison to invasive coronary angiography (ICA).
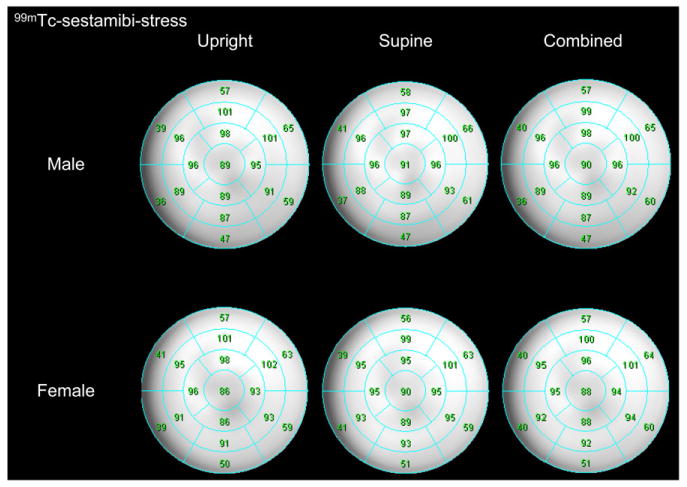
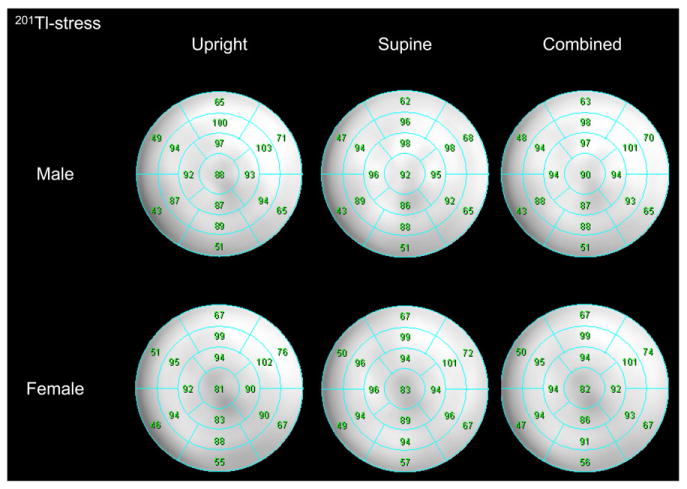
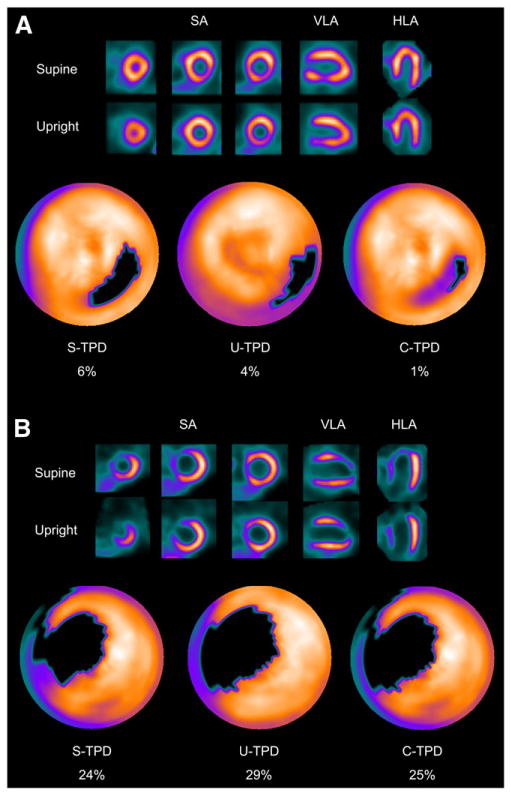
Methods: We studied 142 patients undergoing upright and supine HS-SPECT, including 56 consecutive patients (63% men; mean age ± SD, 64 ± 13 y; 45% exercise stress) without known CAD who underwent diagnostic ICA within 6 mo of HS-SPECT and 86 consecutive patients with a low likelihood of CAD. Reference limits for upright and supine HS-SPECT were created from studies of patients with a low likelihood of CAD. Automated software adopted from supine-prone analysis was used to quantify the severity and extent of perfusion abnormality and was expressed as total perfusion deficit (TPD). TPD was obtained for upright (U-TPD), supine (S-TPD), and combined upright-supine acquisitions (C-TPD). Stress U-TPD ≥ 5%, S-TPD ≥ 5%, and C-TPD ≥ 3% myocardium were considered abnormal for per-patient analysis, and U-TPD, S-TPD, and C-TPD ≥ 2% in each coronary artery territory were considered abnormal for per-vessel analysis.
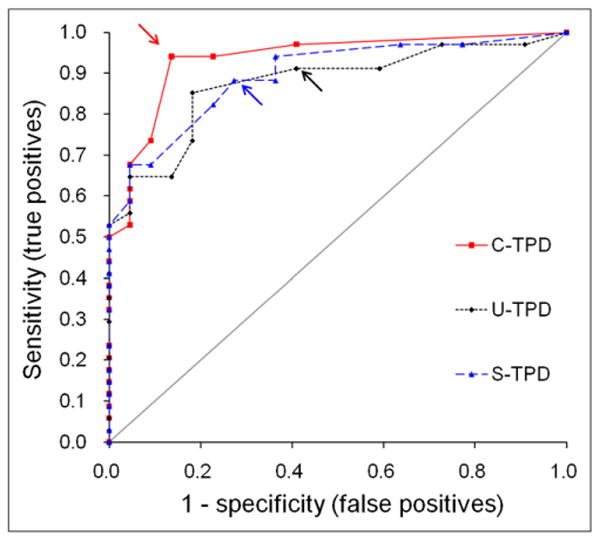
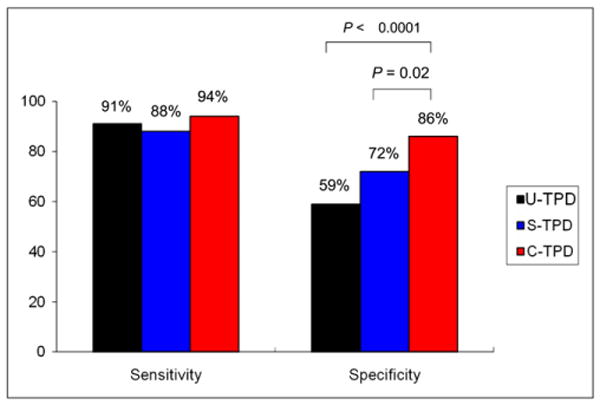
Results: On a per-patient basis, the sensitivity was 91%, 88%, and 94% for U-TPD, S-TPD, and C-TPD, respectively, and specificity was 59%, 73%, and 86% for U-TPD, S-TPD, and C-TPD, respectively. C-TPD had a larger area under the receiver-operating-characteristic curve than U-TPD or S-TPD for identification of stenosis ≥ 70% (0.94 vs. 0.88 and 0.89, P < 0.05 and not significant, respectively). On a per-vessel basis, the sensitivity was 67%, 66%, and 69% for U-TPD, S-TPD, and C-TPD, respectively, and specificity was 91%, 94%, and 97% for U-TPD, S-TPD, and C-TPD, respectively (P = 0.02 for specificity U-TPD vs. C-TPD).
Conclusion: In this first comparison of HS-SPECT with ICA, new automated quantification of combined upright and supine HS-SPECT shows high diagnostic accuracy for detecting clinically significant CAD, with findings comparable to those reported using conventional SPECT.
Figures
References
-
- Slomka PJ, Patton JA, Berman DS, Germano G. Advances in technical aspects of myocardial perfusion SPECT imaging. J Nucl Cardiol. 2009;16:255–276. - PubMed
-
- Patton J, Slomka P, Germano G, Berman DS. Recent technological advances in nuclear cardiology. J Nucl Cardiol. 2007;14:501–513. - PubMed
-
- Sharir T, Ben-Haim S, Merzon K, et al. High-speed myocardial perfusion imaging: initial clinical comparison with conventional dual detector Anger camera imaging. JACC Cardiovasc Imaging. 2008;1:156–163. - PubMed
-
- Gambhir SS, Berman DS, Ziffer J, et al. A novel high-sensitivity rapid-acquisition single-photon cardiac imaging camera. J Nucl Med. 2009;50:635–643. - PubMed
-
- Sharir T, Slomka PJ, Hayes SW, et al. Multicenter trial of high-speed versus conventional SPECT imaging: quantitative results of myocardial perfusion and left ventricular function. J Am Coll Cardiol. 2010;55:1965–1974. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous