

Impact of overall treatment time on survival and local control in patients with anal cancer: a pooled data analysis of Radiation Therapy Oncology Group trials 87-04 and 98-11
- PMID: 20956625
- PMCID: PMC3018356
- DOI: 10.1200/JCO.2010.29.1351
Impact of overall treatment time on survival and local control in patients with anal cancer: a pooled data analysis of Radiation Therapy Oncology Group trials 87-04 and 98-11
Abstract
Purpose: To determine whether increased duration of radiation therapy (RT) and overall treatment (RX) time has a detrimental effect in anal cancer.
Patients and methods: Data from Radiation Therapy Oncology Group (RTOG) 87-04 and RTOG 98-11 trials were combined to form three treatment groups: RT/fluorouracil (FU)/mitomycin (n = 472), RT/FU/cisplatin (n = 320), and RT/FU (n = 145). Cox proportional hazards models were used with the following variables: RT duration, RT intensity, RX duration, treatment group, age, sex, Karnofsky performance score (KPS), T stage, N stage, and RT dose.
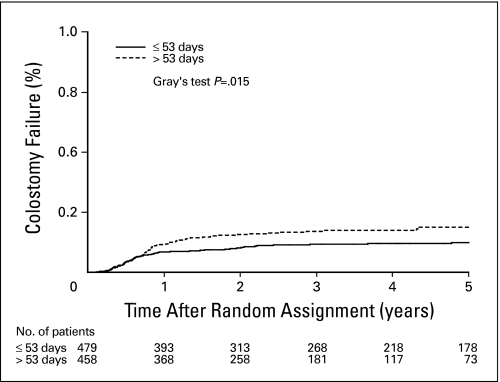
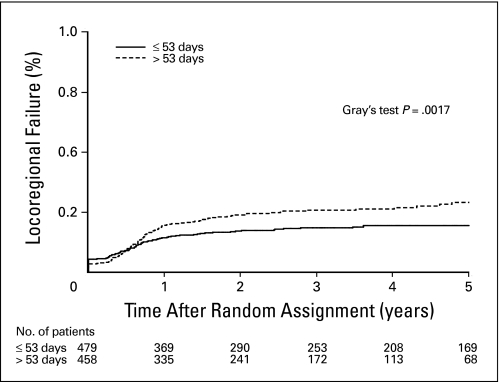
Results: In the univariate analysis, there was a significant association between RX duration and colostomy failure (CF; hazard ratio [HR] = 1.51; 95% CI, 1.07 to 2.14; P = .02), local failure (HR = 1.52; 95% CI, 1.14 to 2.03; P = .005), locoregional failure (HR = 1.51; 95% CI, 1.15 to 1.98; P = .003), and time to failure (HR = 1.40; 95% CI, 1.10 to 1.79; P = .007). The significance of RX duration was maintained after adjusting for treatment group. In multivariate modeling there was a trend toward an association between RX duration and CF (HR = 1.57; 95% CI, 0.98 to 2.50; P = .06) and a statistically significant association with local failure (HR = 1.96; 95% CI, 1.34 to 2.87; P = .0006). Age, sex, KPS, T stage, N stage, and RT dose, but not RT duration, RT intensity, or RX duration, were found to be statistically significant predictors of OS and colostomy-free survival.
Conclusion: Total treatment time, but not duration of radiation therapy, seems to have a detrimental effect on local failure and colostomy rate in anal cancer. Induction chemotherapy may contribute to local failure by increasing total treatment time.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Withers HR, Peters LJ, Taylor JM, et al. Local control of carcinoma of the tonsil by radiation therapy: An analysis of patterns of fractionation in nine institutions. Int J Radiat Oncol Biol Phys. 1995;33:549–562. - PubMed
-
- Withers HR, Taylor JM, Maciejewski B. The hazard of accelerated tumor clonogen repopulation during radiotherapy. Acta Oncol. 1988;27:131–146. - PubMed
-
- Nguyen LN, Ang KK. Radiotherapy for cancer of the head and neck: Altered fractionation regimens. Lancet Oncol. 2002;3:693–701. - PubMed
-
- Bourhis J, Overgaard J, Audry H, et al. Hyperfractionated or accelerated radiotherapy in head and neck cancer: A meta-analysis. Lancet. 2006;368:843–854. - PubMed
-
- Chen SW, Liang JA, Yang SN, et al. The adverse effect of treatment prolongation in cervical cancer by high-dose-rate intracavitary brachytherapy. Radiother Oncol. 2003;67:69–76. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
