

Ductal carcinoma in situ: risk factors and impact of screening
- PMID: 20956813
- PMCID: PMC5161075
- DOI: 10.1093/jncimonographs/lgq024
Ductal carcinoma in situ: risk factors and impact of screening
Abstract
Background: The National Institutes of Health Office of Medical Applications of Research commissioned a structured literature review on the incidence of ductal carcinoma in situ (DCIS) as a background paper for the State of the Science Conference on Diagnosis and Management of DCIS.
Methods: Published studies were abstracted from MEDLINE and other sources. We include articles published through January 31, 2009; 92 publications were abstracted.
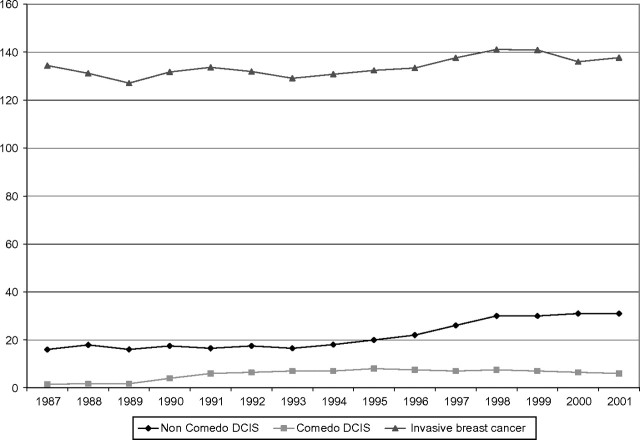
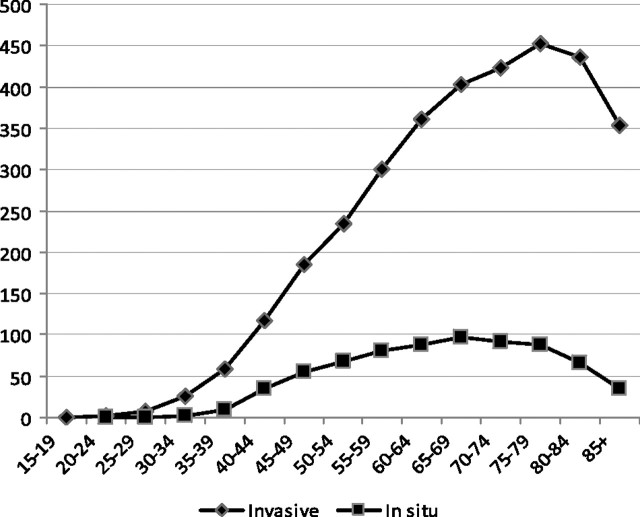
Results: DCIS incidence rose from 1.87 per 100,000 in 1973-1975 to 32.5 per 100,000 in 2005. Increases in incidence were greatest in tumors without comedo necrosis. Incidence increased in all ages but more in women older than 50 years. Increased use of mammography explains some but not all of the increased incidence. Risk factors for incident DCIS include older age and positive family history. Whereas tamoxifen prevents both invasive breast cancer and DCIS, raloxifene is associated with decreased invasive breast cancer but not decreased DCIS.
Conclusions: Scientific questions deserving further investigation include the relationship between mammography use and DCIS incidence and the role of chemoprevention for reducing the incidence of DCIS and invasive breast cancer.
Figures
References
-
- Ries LaG, Melbert D, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2005. Bethesda, MD: National Cancer Institute; 2008. http://seer.cancer.gov/csr/1975_2005/Accessed March 28, 2010.
-
- Li CI, Daling JR, Malone KE. Age-specific incidence rates of in situ breast carcinomas by histologic type, 1980 to 2001. Cancer Epidemiol Biomarkers Prev. 2005;14(4):1008–1011. - PubMed
-
- Innos K, Horn-Ross PL. Recent trends and racial/ethnic differences in the incidence and treatment of ductal carcinoma in situ of the breast in California women. Cancer. 2003;97(4):1099–1106. - PubMed
-
- Wohlfahrt J, Rank F, Kroman N, et al. A comparison of reproductive risk factors for CIS lesions and invasive breast cancer. Int J Cancer. 2004;108(5):750–753. - PubMed
-
- Kerlikowske K, Barclay J, Grady D, et al. Comparison of risk factors for ductal carcinoma in situ and invasive breast cancer. J Natl Cancer Inst. 1997;89(1):76–82. - PubMed
