

Review
doi: 10.1093/jncimonographs/lgq035.
Ductal carcinoma in situ: terminology, classification, and natural history
Affiliations
- PMID: 20956817
- PMCID: PMC5161057
- DOI: 10.1093/jncimonographs/lgq035
Item in Clipboard
Review
Ductal carcinoma in situ: terminology, classification, and natural history
J Natl Cancer Inst Monogr.
2010.
Abstract
Ductal carcinoma in situ (DCIS) refers to breast epithelial cells that have become "cancerous" but still reside in their normal place in the ducts and lobules. In this setting, cancerous means that there is an abnormal increase in the growth of the epithelial cells, which accumulate within and greatly expand the ducts and lobules. DCIS is a nonlethal type of cancer because it stays in its normal place. However, DCIS is very important because it is the immediate precursor of invasive breast cancers, which are potentially lethal. This article provides a general overview of DCIS, including historical perspective, methods of classification, current perspective, and future goals.
Figures
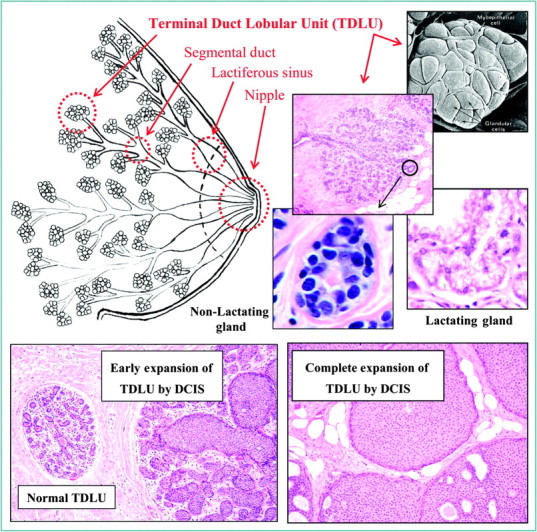
The female human breast is composed of thousands of grape-like clusters of small glands lined by epithelial cells that produce milk, referred to as terminal duct lobular units (TDLUs). The milk is propagated outward through a series of interconnecting and increasingly large ducts that exit the nipple. Ductal carcinoma in situ (DCIS) refers to breast epithelial cells that have become “cancerous” but still reside in their normal place. In this setting, cancerous means that there is an abnormal increase in the growth of the epithelial cells, which accumulate within and greatly expand the glands and ducts.
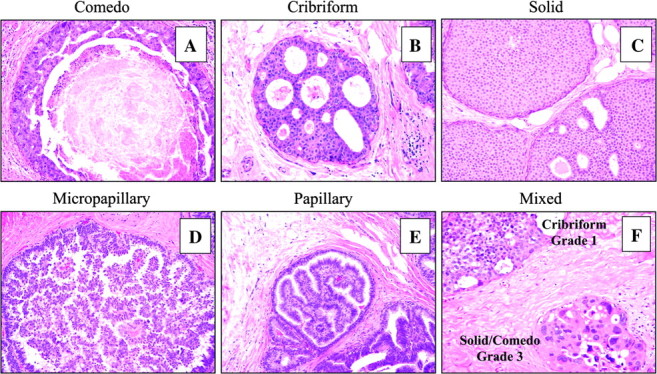
A historical method of classifying ductal carcinoma in situ (DCIS) is based on their predominant microscopic growth pattern and includes comedo (A), cribriform (B), solid (C), micropapillary (D), and papillary (E) subtypes. However, a large proportion of DCIS shows complex mixtures of growth patterns (F), which is difficult to categorize.
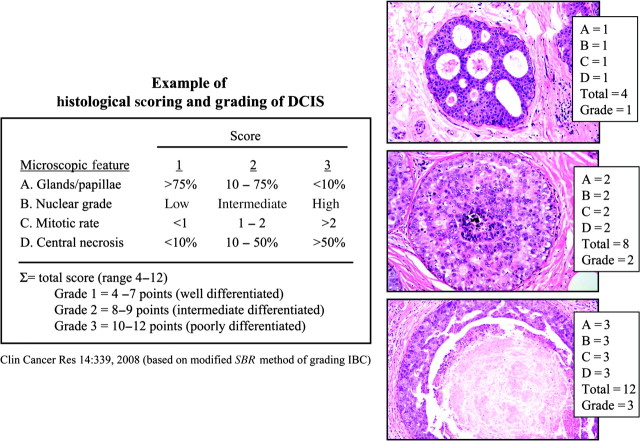
A relatively recent approach to classifying ductal carcinoma in situ is based on the degree that the tumor cells resemble normal cells (referred to as differentiation), and the rate the cells are proliferating. Histological grading systems have been developed, which assign scores or points to convey the magnitude of certain cellular features in the tumor, such as the degree of gland or papillae formation, nuclear size and shape, mitotic rate, and the amount of central necrosis. There are several methods and their details vary, but most recognize three grades corresponding to well (grade 1), moderately (grade 2), and poorly (grade 3) differentiated. However, there is no accepted standard method of grading. DCIS = ductal carcinoma in situ.
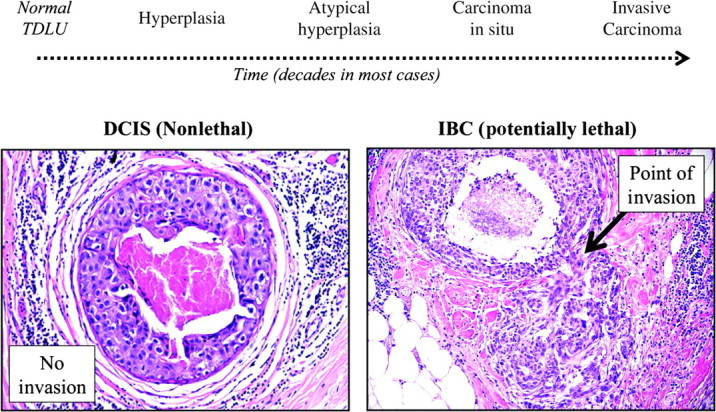
Invasive breast cancers (IBCs) are thought to evolve through a nonobligatory series of increasingly abnormal “stages,” referred to as hyperplasia, atypical hyperplasia, and carcinoma in situ over long periods of time, probably decades in most cases. Ductal carcinoma in situ (DCIS) is the main type of carcinoma in situ in the breast (80%–90%) and a late stage of breast cancer evolution. Many types of evidence support the hypothesis that DCIS are the immediate precursor of IBCs, including points of histological continuity (right photomicrograph).
References
-
- Osborne MP. Breast anatomy and development. In: Harris JR, Lippman ME, Morrow M, Osborne CK, editors; Harris JRLM, Morrow M, Hellman S, Osborne CK, translators. Diseases of the Breast. 3rd ed. Philadelphia, PA: Lippincott, Williams and Wilkins; 2004. pp. 3–14. trans.
-
- Allred DC. Biological characteristics of ductal carcinoma in situ. In: Silverstein ML, editor. Ductal Carcinoma In Situ of the Breast. 2nd ed. Philadelphia, PA: Lipincott: Williams and Wilkins; 2002. pp. 37–48.
-
- Wellings RR, Jensen HM. On the origin and progression of ductal carcinoma in the human breast. J Natl Cancer Inst. 1973;50(5):1111–1118. - PubMed
-
- Allred DC. Biological features of human premalignant breast disease and the progression to cancer. In: Harris JR, Lippman ME, Morrow M, Osborne CK, editors. Diseases of the Breast. 4th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2009. pp. 323–334.
-
- Cheatle GL, Cutler M. Malignant epithelial neoplasia. Carcinoma. The precancerous or potentially carcinomatous state. In: Cheatle GL, Cutler M, editors. Tumours of the Breast. 1st ed. Philadelphia, PA: Lippincott; 1926. pp. 161–332.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
