

Local and systemic outcomes in DCIS based on tumor and patient characteristics: the radiation oncologist's perspective
- PMID: 20956825
- PMCID: PMC5161077
- DOI: 10.1093/jncimonographs/lgq025
Local and systemic outcomes in DCIS based on tumor and patient characteristics: the radiation oncologist's perspective
Abstract
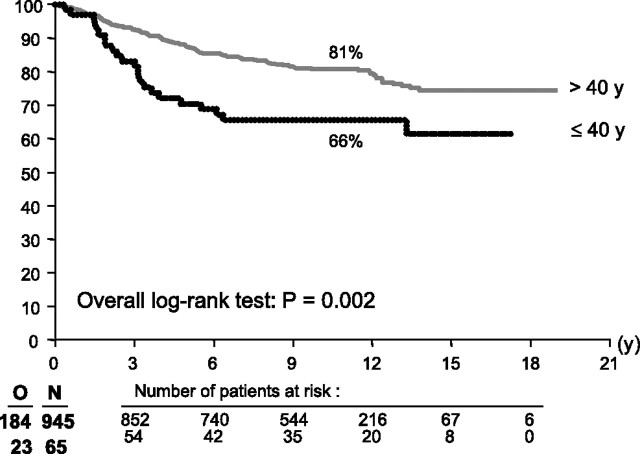
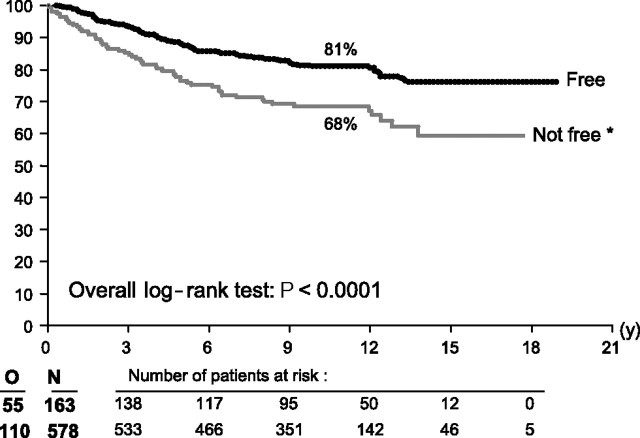
Four randomized clinical trials have shown unanimously the benefit of 50 Gy whole-breast radiotherapy in breast-conserving therapy (BCT) for ductal carcinoma in situ (DCIS). The risk of both DCIS and invasive local recurrence is reduced with about 50%, and this effect is similar for all clinical and histological subgroups analyzed. Younger age and involved margin status are the most important factors for an increased risk of local recurrence. In these subgroups, even with radiotherapy, the observed local recurrence rates are more than 20% at 10 years, which is considerably higher than reported local recurrence rates after BCT for invasive breast cancer. The optimal radiotherapy dose in BCT for DCIS has yet to be established. Also, at present, a subgroup of lesions in which the recurrence rate is so low that radiotherapy can be safely omitted has not yet been identified.
Figures
Similar articles
-
The impact of adding radiation treatment after breast conservation surgery for ductal carcinoma in situ of the breast.J Natl Cancer Inst Monogr. 2010;2010(41):187-92. doi: 10.1093/jncimonographs/lgq020. J Natl Cancer Inst Monogr. 2010. PMID: 20956827 Free PMC article. Review.
-
Overview of the randomized trials of radiotherapy in ductal carcinoma in situ of the breast.J Natl Cancer Inst Monogr. 2010;2010(41):162-77. doi: 10.1093/jncimonographs/lgq039. J Natl Cancer Inst Monogr. 2010. PMID: 20956824 Free PMC article. Review.
-
The impact of surgery, radiation, and systemic treatment on outcomes in patients with ductal carcinoma in situ.J Natl Cancer Inst Monogr. 2010;2010(41):130-3. doi: 10.1093/jncimonographs/lgq022. J Natl Cancer Inst Monogr. 2010. PMID: 20956816 Free PMC article. Review.
-
The impact of systemic therapy following ductal carcinoma in situ.J Natl Cancer Inst Monogr. 2010;2010(41):200-3. doi: 10.1093/jncimonographs/lgq021. J Natl Cancer Inst Monogr. 2010. PMID: 20956830 Free PMC article. Review.
-
The impact of surgery on ductal carcinoma in situ outcomes: the use of mastectomy.J Natl Cancer Inst Monogr. 2010;2010(41):197-9. doi: 10.1093/jncimonographs/lgq032. J Natl Cancer Inst Monogr. 2010. PMID: 20956829 Free PMC article. Review.
Cited by
-
Long-term outcomes of ductal carcinoma in situ of the breast: a systematic review, meta-analysis and meta-regression analysis.BMC Cancer. 2015 Nov 10;15:890. doi: 10.1186/s12885-015-1904-7. BMC Cancer. 2015. PMID: 26555555 Free PMC article.
-
DEGRO practical guidelines: radiotherapy of breast cancer II: radiotherapy of non-invasive neoplasia of the breast.Strahlenther Onkol. 2014 Jan;190(1):8-16. doi: 10.1007/s00066-013-0502-3. Strahlenther Onkol. 2014. PMID: 24306068
-
Breast carcinoma in situ: An observational study of tumor subtype, treatment and outcomes.Oncotarget. 2017 Jan 10;8(2):2361-2371. doi: 10.18632/oncotarget.13785. Oncotarget. 2017. PMID: 27926499 Free PMC article.
-
Role of the radiotherapy boost on local control in ductal carcinoma in situ.Int J Surg Oncol. 2012;2012:748196. doi: 10.1155/2012/748196. Epub 2012 Apr 8. Int J Surg Oncol. 2012. PMID: 22577533 Free PMC article.
-
Basal cytokeratin as a potential marker of low risk of invasion in ductal carcinoma in situ.Clinics (Sao Paulo). 2013 May;68(5):638-43. doi: 10.6061/clinics/2013(05)010. Clinics (Sao Paulo). 2013. PMID: 23778411 Free PMC article.
References
-
- Fisher B, Land S, Mamounas E, Dignam J, Fisher ER, Wolmark N. Prevention of invasive breast cancer in women with ductal carcinoma in situ: an update of the National Surgical Adjuvant Breast and Bowel Project experience. Semin Oncol. 2001;28(4):400–418. - PubMed
-
- Bijker N, Meijnen P, Peterse JL, et al. Breast-conserving treatment with or without radiotherapy in ductal carcinoma-in-situ: ten-year results of European Organisation for Research and Treatment of Cancer randomized phase III trial 10853—a study by the EORTC Breast Cancer Cooperative Group and EORTC Radiotherapy Group. J Clin Oncol. 2006;24(21):3381–3387. - PubMed
-
- Houghton J, George WD, Cuzick J, Duggan C, Fentiman IS, Spittle M. UK Coordinating Committee on Cancer Research; Ductal Carcinoma in situ Working Party; DCIS trialists in the UK, Australia, and New Zealand. Radiotherapy and tamoxifen in women with completely excised ductal carcinoma in situ of the breast in the UK, Australia, and New Zealand: randomised controlled trial. Lancet. 2003;362(9378):95–102. - PubMed
-
- Holmberg L, Garmo H, Granstrand B, et al. Absolute risk reductions for local recurrence after postoperative radiotherapy after sector resection for ductal carcinoma in situ of the breast. J Clin Oncol. 2008;26(8):1247–1252. - PubMed
-
- Goodwin A, Parker S, Ghersi D, Wilcken N. Post-operative radiotherapy for ductal carcinoma in situ of the breast. Cochrane Database Syst Rev. 2009;21(1) CD000563. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
