

Review
doi: 10.1093/jncimonographs/lgq037.
Imaging for the diagnosis and management of ductal carcinoma in situ
Affiliations
- PMID: 20956833
- PMCID: PMC5161079
- DOI: 10.1093/jncimonographs/lgq037
Item in Clipboard
Review
Imaging for the diagnosis and management of ductal carcinoma in situ
J Natl Cancer Inst Monogr.
2010.
Abstract
Diagnosis of ductal carcinoma in situ (DCIS) has increased dramatically in parallel with the increased use of screening mammography. There are specific mammographic findings, most associated with shapes (amorphous, fine and coarse pleomorphic, and fine linear) and distributions (linear and segmental) of calcifications that permit a reasonable sensitivity for detection of DCIS without an unreasonable decrease in specificity, especially in view of the dramatic decrease in breast cancer mortality associated with early detection. While some DCIS may never progress to invasive disease, at this time, we cannot make that separation. This should be an active area for research.
Figures
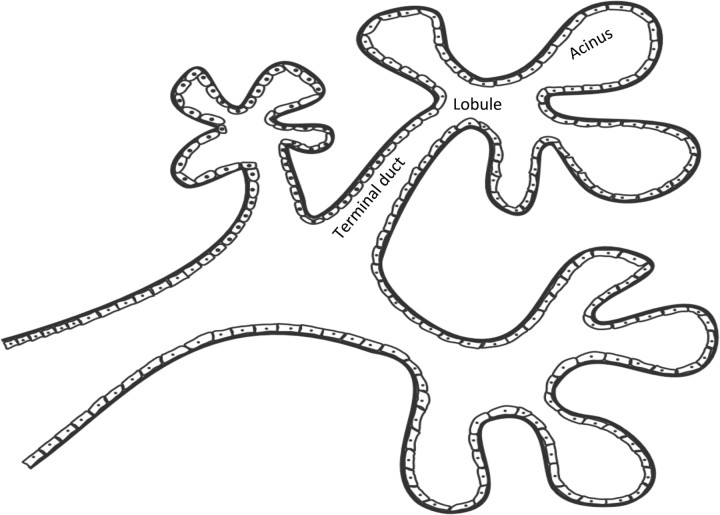
Terminal ductal lobular unit. The basic subgross histological unit in the breast is the terminal ductal lobular unit. There is a terminal duct and a lobule. The lobule is subdivided into acini.
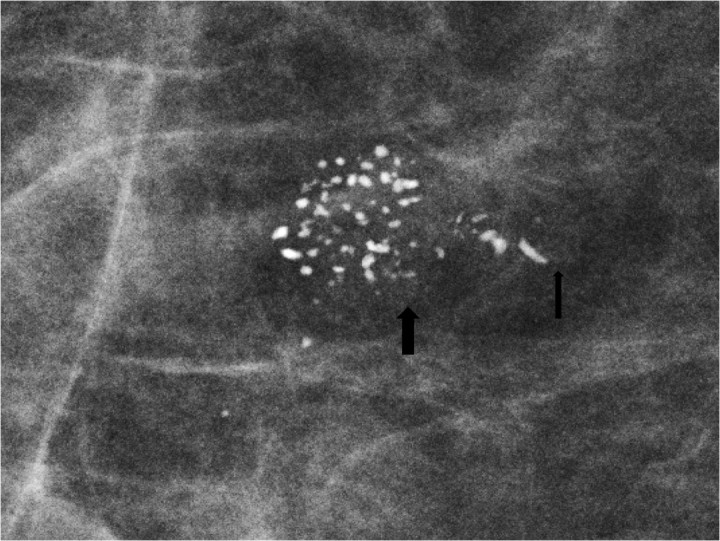
Spot magnification mammogram. The anatomy of the terminal ductal lobular unit is demonstrated on this magnification spot view with the lobule and acini filled with coarse heterogeneous calcifications (large arrow) and the terminal duct filled with linear forms of calcifications (small arrow). Pathology: comedo ductal carcinoma in situ.
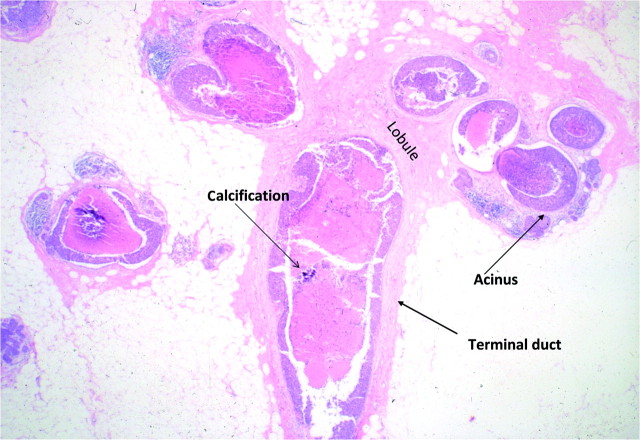
Histology of terminal ductal lobular unit.
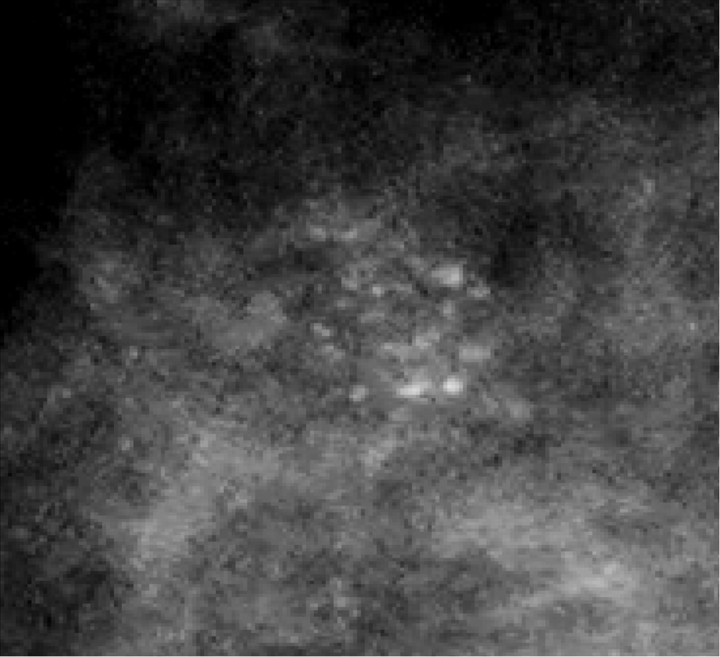
Spot magnification mammogram. Cluster of amorphous calcifications. Note the hazy appearance of these calcifications. Pathology: cribiform ductal carcinoma in situ.
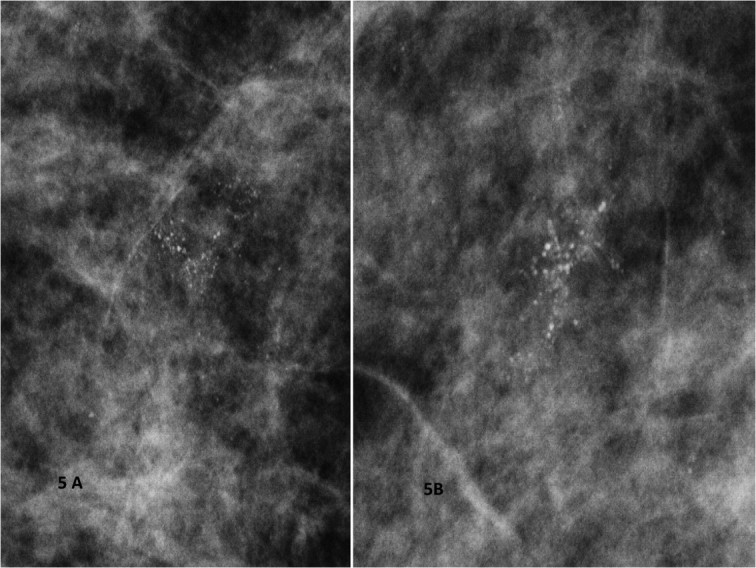
A) and B) Spot magnification mammograms. Two different patients with a segmental arrangement of fine pleomorphic calcifications. Pathology: comedo ductal carcinoma in situ.
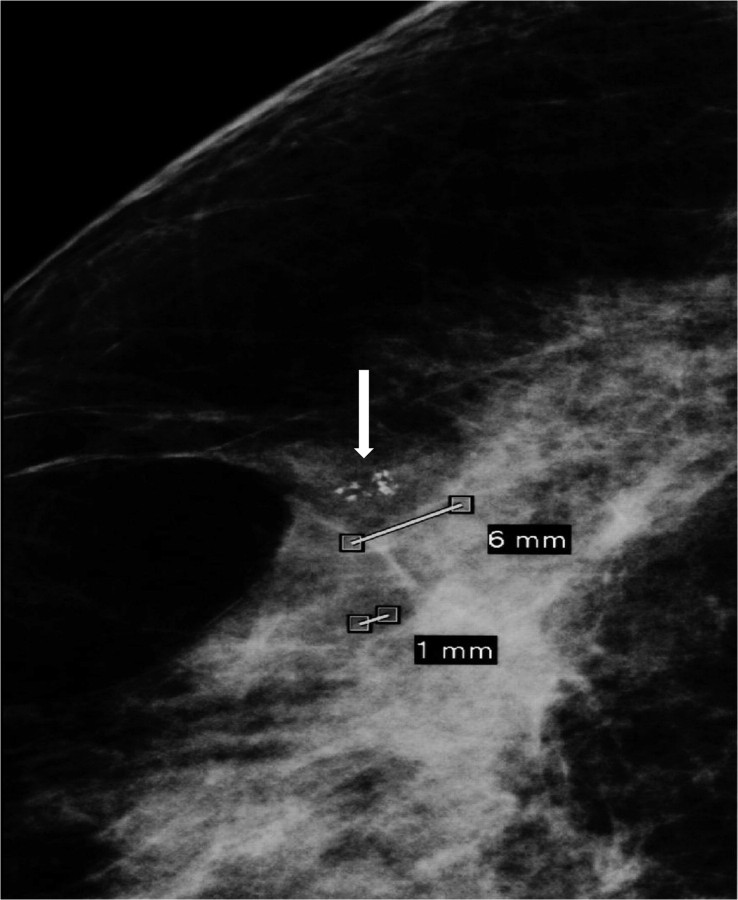
Spot magnification mammography. Cluster of coarse hetereogeneous calcifications. Note size of the individual particles approaching 1 mm (arrow). Pathology: benign fibroadenomatoid change.
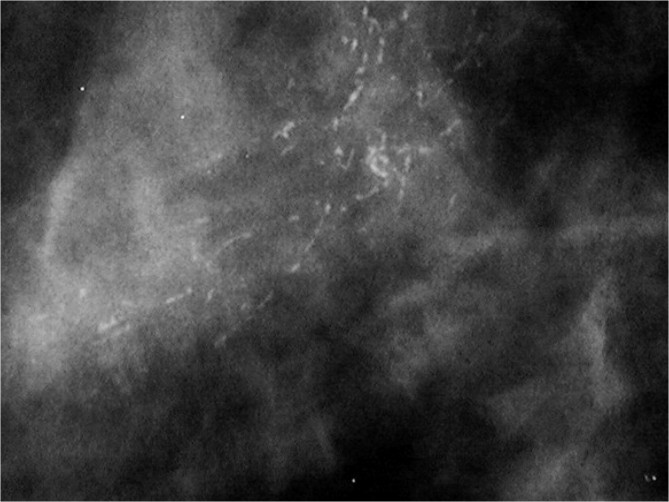
Spot magnification mammogram. A segmental arrangement of fine linear calcifications. Pathology: comedo ductal carcinoma in situ.
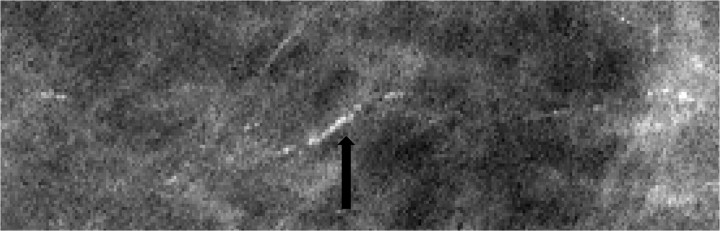
Spot magnification mammogram. Linear arrangement of punctate calcifications. Pathology: cribiform ductal carcinoma in situ.
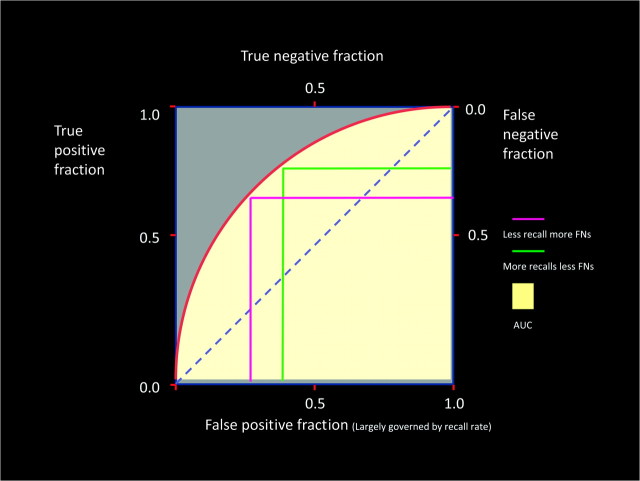
Receiver operating characteristic curve.
References
-
- Blichert-Toft M, Graversen HP, Andersen J, et al. In sity breast carcinomas: a population-based study on frequency, growth pattern, and clinical aspects. World J Surg. 1988;12:845–851. - PubMed
-
- Ward BA, McKhann CF, Ravikumar TS. Ten-year follow-up of breast carcinoma in situ in Connecticut. Arch Surg. 1992;127(12):1392–1395. - PubMed
-
- Barreau B, deMascarel I, Feuga C, et al. Mammography of ductal carcinoma in situ of the breast: review of 909 cases with radiographic-pathologic correlation. Eur J Radiol. 2005;54(1):55–61. - PubMed
-
- Tabar L, Duffy SW, Burhenne LW, et al. New Swedish breast cancer detection results for women aged 40-49. Cancer. 1993;72(4 suppl):1437–1448. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
