

Computational modeling of fluid flow and intra-ocular pressure following glaucoma surgery
- PMID: 20957178
- PMCID: PMC2949396
- DOI: 10.1371/journal.pone.0013178
Computational modeling of fluid flow and intra-ocular pressure following glaucoma surgery
Abstract
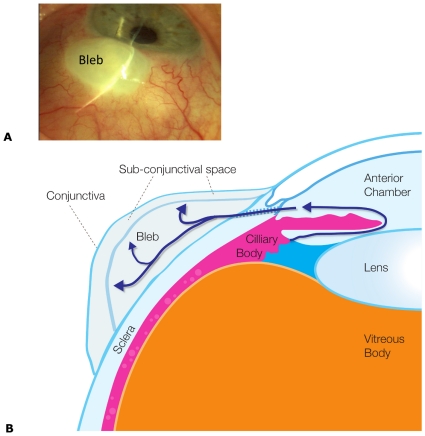
Background: Glaucoma surgery is the most effective means for lowering intraocular pressure by providing a new route for fluid to exit the eye. This new pathway is through the sclera of the eye into sub-conjunctival tissue, where a fluid filled bleb typically forms under the conjunctiva. The long-term success of the procedure relies on the capacity of the sub-conjunctival tissue to absorb the excess fluid presented to it, without generating excessive scar tissue during tissue remodeling that will shut-down fluid flow. The role of inflammatory factors that promote scarring are well researched yet little is known regarding the impact of physical forces on the healing response.
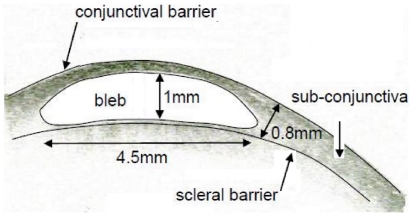
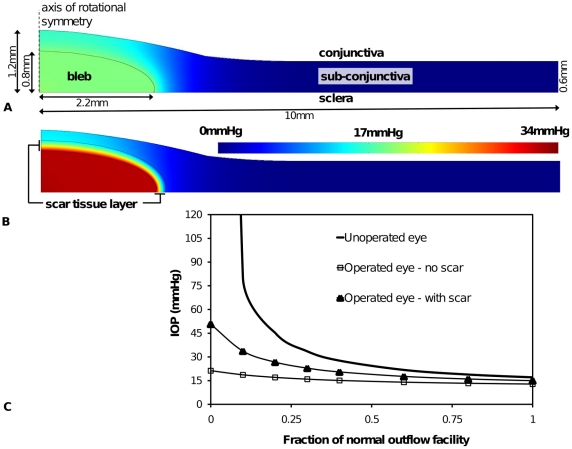
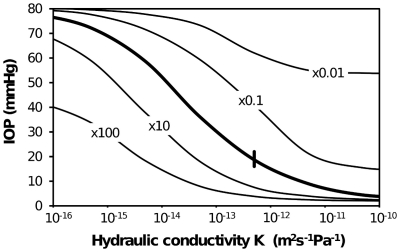
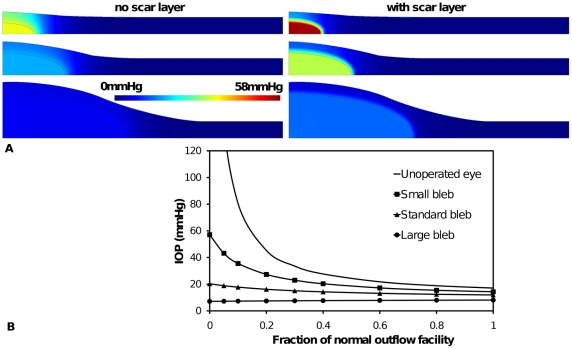
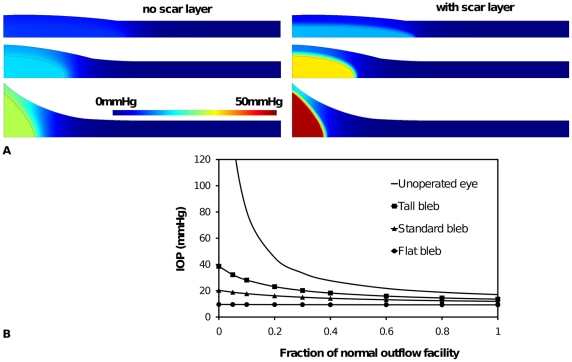
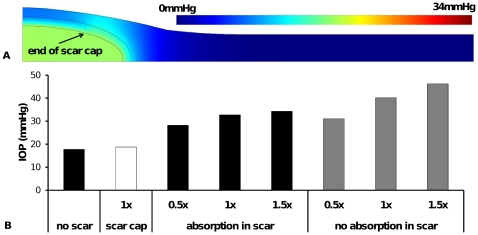
Methodology: To help elucidate the interplay of physical factors controlling the distribution and absorption of aqueous humor in sub-conjunctival tissue, and tissue remodeling, we have developed a computational model of fluid production in the eye and removal via the trabecular/uveoscleral pathways and the surgical pathway. This surgical pathway is then linked to a porous media computational model of a fluid bleb positioned within the sub-conjunctival tissue. The computational analysis is centered on typical functioning bleb geometry found in a human eye following glaucoma surgery. A parametric study is conducted of changes in fluid absorption by the sub-conjunctival blood vessels, changes in hydraulic conductivity due to scarring, and changes in bleb size and shape, and eye outflow facility.
Conclusions: This study is motivated by the fact that some blebs are known to have 'successful' characteristics that are generally described by clinicians as being low, diffuse and large without the formation of a distinct sub-conjunctival encapsulation. The model predictions are shown to accord with clinical observations in a number of key ways, specifically the variation of intra-ocular pressure with bleb size and shape and the correspondence between sites of predicted maximum interstitial fluid pressure and key features observed in blebs, which gives validity to the model described here. This model should contribute to a more complete explanation of the physical processes behind successful bleb characteristics and provide a new basis for clinically grading blebs.
Conflict of interest statement
Figures
References
-
- Hong C-H, Arosemena A, Zurakowski D, Ayyala RS. Glaucoma Drainage Devices: A Systematic Literature Review and Current Controversies. Survey of Ophthalmology. 2005;50:48–60. - PubMed
-
- Wells AP, Ashraff NN, Hall RC, Purdie G. Comparison of Two Clinical Bleb Grading Systems. Ophthalmology. 2006;113:77–83. - PubMed
-
- Azuara-Blanco A, Katz LJ. Dysfunctional filtering blebs. Survey of Opthalmology. 1998;43:93–126. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
