

Acute-phase reactants and a supplemental diagnostic aid for Kawasaki disease
- PMID: 20957478
- PMCID: PMC3933282
- DOI: 10.1007/s00246-010-9801-y
Acute-phase reactants and a supplemental diagnostic aid for Kawasaki disease
Abstract
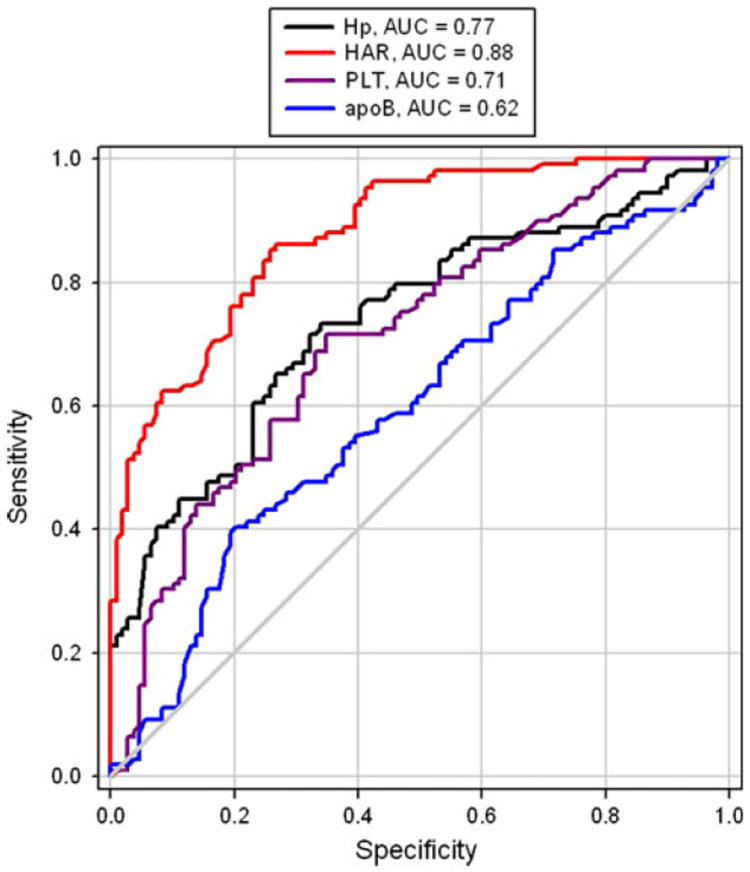
The diagnosis of acute Kawasaki disease (KD) is based on characteristic clinical signs and not on a specific diagnostic test. The authors performed a comprehensive evaluation of acute-phase reactants in KD to determine which of the acute-phase reactants would most accurately distinguish KD from other febrile illnesses. Blood was collected from 218 cases of febrile children with KD (64 cases); bacterial pneumonia (74 cases); hand, foot, and mouth disease (31 cases); and upper respiratory tract infection (49 cases) in acute-stage illness before any therapy. The demographics, body temperature, and laboratory markers including white blood cell count, red blood cell count, and levels of hemoglobin, platelets, C-reactive protein, haptoglobin, apolipoprotein A-I, and apolipoprotein B were evaluated. Using post hoc analysis, the platelet count (10(3)/μl) and haptoglobin/apolipoprotein A-I ratio were significantly higher for the KD patients (404.64 ± 161.68, P = 0.004; 4.74 ± 2.73, P < 0.001) than for the other groups including patients with pneumonia (272.76 ± 115.07, 2.03 ± 1.88); hand, foot, and mouth disease (274 ± 105.9, 2.24 ± 1.19); and upper respiratory tract infection (282.06 ± 107.72, 1.4 ± 0.98). The best cutoff value of the haptoglobin/apolipoprotein A-I ratio obtained from receiver operating characteristics (ROC) curves for KD was 2 (area under the ROC curve, 0.88; 95% confidence interval, 0.801-0.955), with a sensitivity of 89.7% and a specificity of 85.6% for detecting KD. Our data indicate that the serum haptoglobin/apolipoprotein A-I ratio could be a useful supplemental laboratory marker for the acute phase of KD.
Figures
Similar articles
-
Differences in GlycA and lipoprotein particle parameters may help distinguish acute kawasaki disease from other febrile illnesses in children.BMC Pediatr. 2016 Sep 5;16(1):151. doi: 10.1186/s12887-016-0688-5. BMC Pediatr. 2016. PMID: 27596163 Free PMC article. Clinical Trial.
-
Pro-brain natriuretic peptide (ProBNP) levels in North Indian children with Kawasaki disease.Rheumatol Int. 2016 Apr;36(4):551-9. doi: 10.1007/s00296-016-3430-6. Epub 2016 Feb 5. Rheumatol Int. 2016. PMID: 26849890
-
Novel data-mining approach identifies biomarkers for diagnosis of Kawasaki disease.Pediatr Res. 2015 Nov;78(5):547-53. doi: 10.1038/pr.2015.137. Epub 2015 Aug 3. Pediatr Res. 2015. PMID: 26237629 Free PMC article.
-
Diagnostic significance of circulating miRNAs in Kawasaki disease in China: Current evidence based on a meta-analysis.Medicine (Baltimore). 2021 Feb 12;100(6):e24174. doi: 10.1097/MD.0000000000024174. Medicine (Baltimore). 2021. PMID: 33578520 Free PMC article.
-
Usefulness of brain natriuretic peptide to distinguish Kawasaki disease from cervical lymphadenitis.Pediatr Int. 2022 Jan;64(1):e15050. doi: 10.1111/ped.15050. Pediatr Int. 2022. PMID: 34739174 Review.
Cited by
-
A New Diagnostic Model to Distinguish Kawasaki Disease From Other Febrile Illnesses in Chongqing: A Retrospective Study on 10,367 Patients.Front Pediatr. 2020 Nov 12;8:533759. doi: 10.3389/fped.2020.533759. eCollection 2020. Front Pediatr. 2020. PMID: 33304865 Free PMC article.
-
Alterations in bile acid metabolites associated with pathogenicity and IVIG resistance in Kawasaki disease.Front Cardiovasc Med. 2025 Feb 20;12:1549900. doi: 10.3389/fcvm.2025.1549900. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40051431 Free PMC article.
-
Point-of-care differentiation of Kawasaki disease from other febrile illnesses.J Pediatr. 2013 Jan;162(1):183-188.e3. doi: 10.1016/j.jpeds.2012.06.012. Epub 2012 Jul 20. J Pediatr. 2013. PMID: 22819274 Free PMC article.
-
Biomarkers for Kawasaki Disease: Clinical Utility and the Challenges Ahead.Front Pediatr. 2019 Jun 18;7:242. doi: 10.3389/fped.2019.00242. eCollection 2019. Front Pediatr. 2019. PMID: 31275907 Free PMC article. Review.
-
Challenges in early diagnosis of Kawasaki disease in the pediatric emergency department: differentiation from adenoviral and invasive pneumococcal disease.Wien Klin Wochenschr. 2018 Apr;130(7-8):264-272. doi: 10.1007/s00508-018-1324-1. Epub 2018 Feb 23. Wien Klin Wochenschr. 2018. PMID: 29476365
References
-
- Cabana VG, Gidding SS, Getz GS, Chapman J, Shulman ST. Serum amyloid A and high-density lipoprotein participate in the acute-phase response of Kawasaki disease. Pediatr Res. 1997;42:651–655. - PubMed
-
- Carter K, Worwood M. Haptoglobin: a review of the major allele frequencies worldwide and their association with diseases. Int J Lab Hematol. 2007;29:92–110. - PubMed
-
- Fiotti N, Giansante C, Ponte E, Delbello C, Calabrese S, Zacchi T, Dobrina A, Guarnieri G. Atherosclerosis and inflammation: patterns of cytokine regulation in patients with peripheral arterial disease. Atherosclerosis. 1999;145:51–60. - PubMed
-
- Gupta M, Noel GJ, Schaefer M, Friedman D, Bussel J, Johann-Liang R. Cytokine modulation with immune gamma-globulin in peripheral blood of normal children and its implications in Kawasaki disease treatment. J Clin Immunol. 2001;21:193–199. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
