

Effect of high flow oxygen on mortality in chronic obstructive pulmonary disease patients in prehospital setting: randomised controlled trial
- PMID: 20959284
- PMCID: PMC2957540
- DOI: 10.1136/bmj.c5462
Effect of high flow oxygen on mortality in chronic obstructive pulmonary disease patients in prehospital setting: randomised controlled trial
Abstract
Objectives: To compare standard high flow oxygen treatment with titrated oxygen treatment for patients with an acute exacerbation of chronic obstructive pulmonary disease in the prehospital setting.
Design: Cluster randomised controlled parallel group trial.
Setting: Ambulance service in Hobart, Tasmania, Australia.
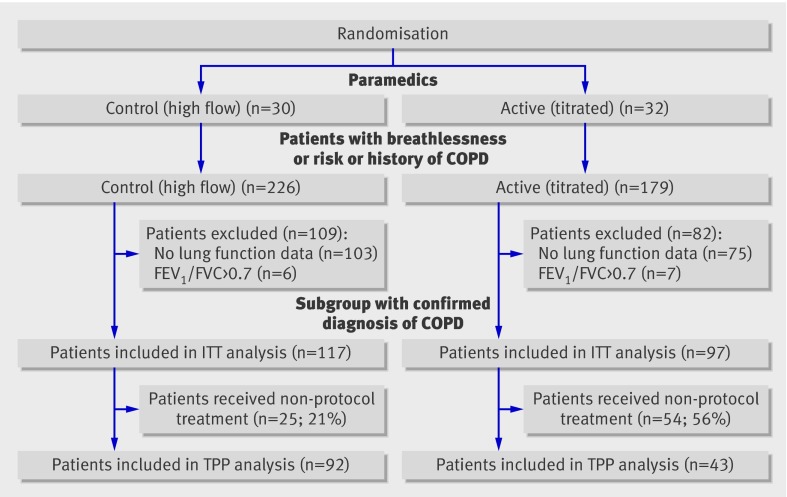
Participants: 405 patients with a presumed acute exacerbation of chronic obstructive pulmonary disease who were treated by paramedics, transported, and admitted to the Royal Hobart Hospital during the trial period; 214 had a diagnosis of chronic obstructive pulmonary disease confirmed by lung function tests in the previous five years.
Interventions: High flow oxygen treatment compared with titrated oxygen treatment in the prehospital (ambulance/paramedic) setting.
Main outcome measure: Prehospital or in-hospital mortality.
Results: In an intention to treat analysis, the risk of death was significantly lower in the titrated oxygen arm compared with the high flow oxygen arm for all patients (high flow oxygen n=226; titrated oxygen n=179) and for the subgroup of patients with confirmed chronic obstructive pulmonary disease (high flow n=117; titrated n=97). Overall mortality was 9% (21 deaths) in the high flow oxygen arm compared with 4% (7 deaths) in the titrated oxygen arm; mortality in the subgroup with confirmed chronic obstructive pulmonary disease was 9% (11 deaths) in the high flow arm compared with 2% (2 deaths) in the titrated oxygen arm. Titrated oxygen treatment reduced mortality compared with high flow oxygen by 58% for all patients (relative risk 0.42, 95% confidence interval 0.20 to 0.89; P=0.02) and by 78% for the patients with confirmed chronic obstructive pulmonary disease (0.22, 0.05 to 0.91; P=0.04). Patients with chronic obstructive pulmonary disease who received titrated oxygen according to the protocol were significantly less likely to have respiratory acidosis (mean difference in pH 0.12 (SE 0.05); P=0.01; n=28) or hypercapnia (mean difference in arterial carbon dioxide pressure -33.6 (16.3) mm Hg; P=0.02; n=29) than were patients who received high flow oxygen.
Conclusions: Titrated oxygen treatment significantly reduced mortality, hypercapnia, and respiratory acidosis compared with high flow oxygen in acute exacerbations of chronic obstructive pulmonary disease. These results provide strong evidence to recommend the routine use of titrated oxygen treatment in patients with breathlessness and a history or clinical likelihood of chronic obstructive pulmonary disease in the prehospital setting.
Trial registration: Australian New Zealand Clinical Trials Register ACTRN12609000236291.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Avoidance of high concentration oxygen in chronic obstructive pulmonary disease.BMJ. 2010 Oct 18;341:c5549. doi: 10.1136/bmj.c5549. BMJ. 2010. PMID: 20959285 No abstract available.
-
Using titrated oxygen instead of high flow oxygen during an acute exacerbation of chronic obstructive pulmonary disease (COPD) saves lives.J Physiother. 2011;57(1):55. doi: 10.1016/S1836-9553(11)70008-X. J Physiother. 2011. PMID: 21402331
References
-
- World Health Organization. Chronic obstructive pulmonary disease (COPD). 2010. www.who.int/respiratory/copd/en/.
-
- American Lung Association. Chronic obstructive pulmonary disease COPD. 2010. www.lungusa.org/assets/documents/publications/solddc-chapters/copd.pdf.
-
- British Lung Foundation. Invisible lives: chronic obstructive pulmonary disease (COPD)—finding the missing millions. British Lung Foundation, 2007 (available at www.lunguk.org/Resources/British%20Lung%20Foundation/Migrated%20Resource...).
-
- Halpern MT, Stanford RH, Borker R. The burden of COPD in the USA: results from the Confronting COPD Survey. Respir Med 2003;97:81-9S. - PubMed
-
- McKenzie D, Frith P, Burdon J, Town G. The COPDX plan: Australian and New Zealand guidelines for the management of chronic obstructive pulmonary disease. Med J Aust 2003;178:1-40S. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical