

Estrogen plus progestin and breast cancer incidence and mortality in postmenopausal women
- PMID: 20959578
- PMCID: PMC5142300
- DOI: 10.1001/jama.2010.1500
Estrogen plus progestin and breast cancer incidence and mortality in postmenopausal women
Abstract
Context: In the Women's Health Initiative randomized, placebo-controlled trial of estrogen plus progestin, after a mean intervention time of 5.6 (SD, 1.3) years (range, 3.7-8.6 years) and a mean follow-up of 7.9 (SD, 1.4) years, breast cancer incidence was increased among women who received combined hormone therapy. Breast cancer mortality among participants in the trial has not been previously reported.
Objective: To determine the effects of therapy with estrogen plus progestin on cumulative breast cancer incidence and mortality after a total mean follow-up of 11.0 (SD, 2.7) years, through August 14, 2009.
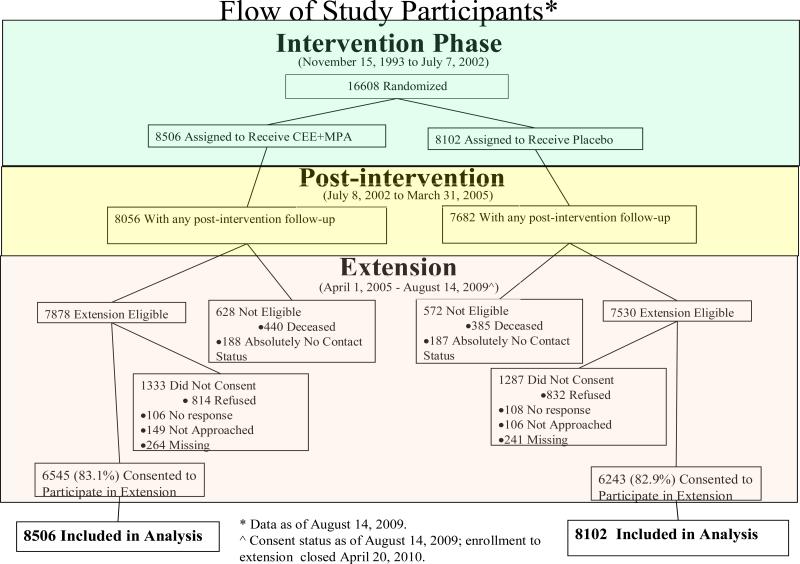
Design, setting, and participants: A total of 16,608 postmenopausal women aged 50 to 79 years with no prior hysterectomy from 40 US clinical centers were randomly assigned to receive combined conjugated equine estrogens, 0.625 mg/d, plus medroxyprogesterone acetate, 2.5 mg/d, or placebo pill. After the original trial completion date (March 31, 2005), reconsent was required for continued follow-up for breast cancer incidence and was obtained from 12,788 (83%) of the surviving participants.
Main outcome measures: Invasive breast cancer incidence and breast cancer mortality.
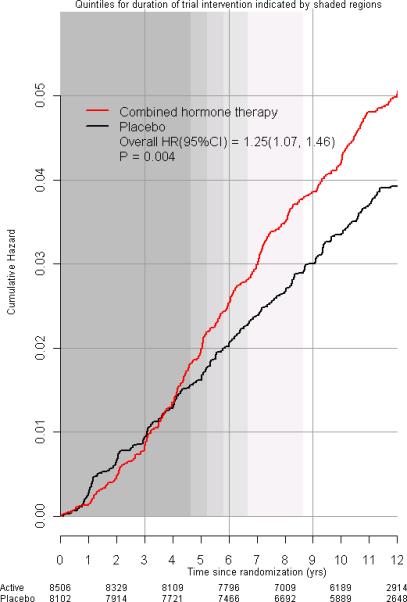
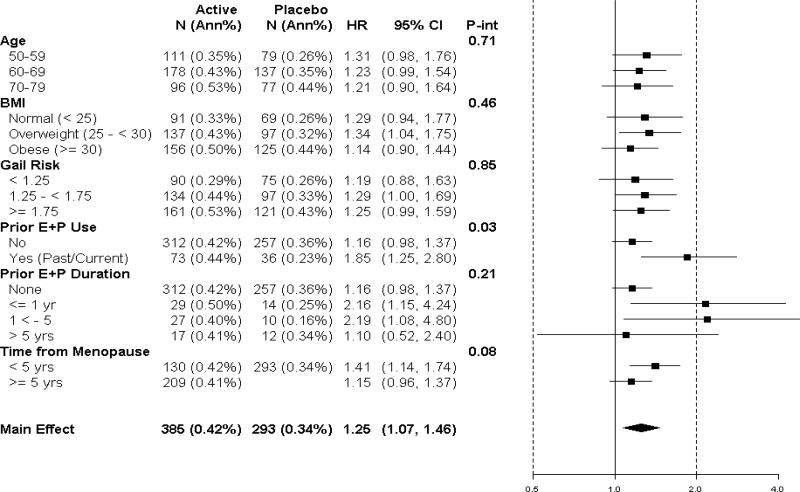
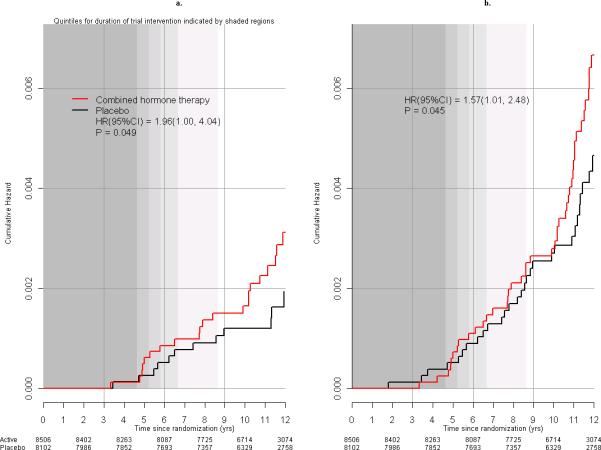
Results: In intention-to-treat analyses including all randomized participants and censoring those not consenting to additional follow-up on March 31, 2005, estrogen plus progestin was associated with more invasive breast cancers compared with placebo (385 cases [0.42% per year] vs 293 cases [0.34% per year]; hazard ratio [HR], 1.25; 95% confidence interval [CI], 1.07-1.46; P = .004). Breast cancers in the estrogen-plus-progestin group were similar in histology and grade to breast cancers in the placebo group but were more likely to be node-positive (81 [23.7%] vs 43 [16.2%], respectively; HR, 1.78; 95% CI, 1.23-2.58; P = .03). There were more deaths directly attributed to breast cancer (25 deaths [0.03% per year] vs 12 deaths [0.01% per year]; HR, 1.96; 95% CI, 1.00-4.04; P = .049) as well as more deaths from all causes occurring after a breast cancer diagnosis (51 deaths [0.05% per year] vs 31 deaths [0.03% per year]; HR, 1.57; 95% CI, 1.01-2.48; P = .045) among women who received estrogen plus progestin compared with women in the placebo group.
Conclusions: Estrogen plus progestin was associated with greater breast cancer incidence, and the cancers are more commonly node-positive. Breast cancer mortality also appears to be increased with combined use of estrogen plus progestin.
Trial registration: clinicaltrials.gov Identifier: NCT00000611.
Figures
Comment in
-
Postmenopausal hormone therapy and breast cancer: an uncertain trade-off.JAMA. 2010 Oct 20;304(15):1719-20. doi: 10.1001/jama.2010.1528. JAMA. 2010. PMID: 20959586 No abstract available.
-
Breast cancer in postmenopausal women after hormone therapy.JAMA. 2011 Feb 2;305(5):466; author reply 466-7. doi: 10.1001/jama.2011.75. JAMA. 2011. PMID: 21285420 No abstract available.
-
Breast cancer in postmenopausal women after hormone therapy.JAMA. 2011 Feb 2;305(5):466; author reply 466-7. doi: 10.1001/jama.2011.74. JAMA. 2011. PMID: 21285421 No abstract available.
-
ACP Journal Club. Estrogen plus progestin increased long-term risk for invasive breast cancer in postmenopausal women.Ann Intern Med. 2011 Feb 15;154(4):JC2-11. doi: 10.7326/0003-4819-154-4-201102150-02011. Ann Intern Med. 2011. PMID: 21320926 No abstract available.
-
New findings from women's health initiative: breast cancer mortality rates higher among combination hormone therapy users.J Midwifery Womens Health. 2011 Mar-Apr;56(2):177-8. doi: 10.1111/j.1542-2011.2010.00054_1.x. J Midwifery Womens Health. 2011. PMID: 21429085 No abstract available.
-
Breast cancer and postmenopausal hormone therapy.Climacteric. 2011 Jun;14(3):400-1. doi: 10.3109/13697137.2011.579039. Climacteric. 2011. PMID: 21563998 No abstract available.
References
-
- Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women's Health Initiative randomized controlled trial. JAMA. 2002;288(3):321–333. - PubMed
-
- Chlebowski RT, Hendrix SL, Langer RD, et al. Influence of estrogen plus progestin on breast cancer and mammography in healthy postmenopausal women: the Women's Health Initiative randomized trial. JAMA. 2003;289(24):3243–3253. - PubMed
-
- Chlebowski RT, Anderson GL, Pettinger M, et al. Estrogen plus progestin and breast cancer detection by means of mammography and breast biopsy. Arch Intern Med. 2008;168(4):370–377. - PubMed
-
- Holi K, Isola J, Cuzick J. Low biologic aggressiveness in breast cancer in women using hormone replacement therapy. J Clin Oncol. 1998;16(9):3115–3120. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- N01WH42119/WH/WHI NIH HHS/United States
- N01WH32106/WH/WHI NIH HHS/United States
- N01WH42131/WH/WHI NIH HHS/United States
- N01WH42109/WH/WHI NIH HHS/United States
- N01WH42114/WH/WHI NIH HHS/United States
- N01 WH032115/WH/WHI NIH HHS/United States
- N01WH42115/WH/WHI NIH HHS/United States
- N01 WH032118/HL/NHLBI NIH HHS/United States
- N01WH42111/WH/WHI NIH HHS/United States
- N01WH32109/WH/WHI NIH HHS/United States
- N01WH42123/WH/WHI NIH HHS/United States
- N01 WH032108/WH/WHI NIH HHS/United States
- N01 WH032119/WH/WHI NIH HHS/United States
- N01WH42124/WH/WHI NIH HHS/United States
- N01WH32102/WH/WHI NIH HHS/United States
- N01 WH044221/WH/WHI NIH HHS/United States
- N01WH42112/WH/WHI NIH HHS/United States
- N01WH32112/WH/WHI NIH HHS/United States
- N01WH32101/WH/WHI NIH HHS/United States
- N01WH42132/WH/WHI NIH HHS/United States
- N01WH42121/WH/WHI NIH HHS/United States
- N01WH42113/WH/WHI NIH HHS/United States
- N01WH42125/WH/WHI NIH HHS/United States
- N01 WH022110/WH/WHI NIH HHS/United States
- N01 WH032100/WH/WHI NIH HHS/United States
- N01 WH032111/WH/WHI NIH HHS/United States
- N01 WH032122/WH/WHI NIH HHS/United States
- N01WH42118/WH/WHI NIH HHS/United States
- N01 WH042107/HL/NHLBI NIH HHS/United States
- N01WH42108/WH/WHI NIH HHS/United States
- N01WH32113/WH/WHI NIH HHS/United States
- N01WH42120/WH/WHI NIH HHS/United States
- N01WH42130/WH/WHI NIH HHS/United States
- N01WH42117/WH/WHI NIH HHS/United States
- N01 WH032105/HL/NHLBI NIH HHS/United States
- N01WH42122/WH/WHI NIH HHS/United States
- N01 WH042129/WH/WHI NIH HHS/United States
- N01 WH024152/WH/WHI NIH HHS/United States
- N01WH42110/WH/WHI NIH HHS/United States
- N01WH42126/WH/WHI NIH HHS/United States
- N01WH42116/WH/WHI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
