

Diagnosing delirium in critically ill children: Validity and reliability of the Pediatric Confusion Assessment Method for the Intensive Care Unit
- PMID: 20959783
- PMCID: PMC3776416
- DOI: 10.1097/CCM.0b013e3181feb489
Diagnosing delirium in critically ill children: Validity and reliability of the Pediatric Confusion Assessment Method for the Intensive Care Unit
Abstract
Objective: To validate a diagnostic instrument for pediatric delirium in critically ill children, both ventilated and nonventilated, that uses standardized, developmentally appropriate measurements.
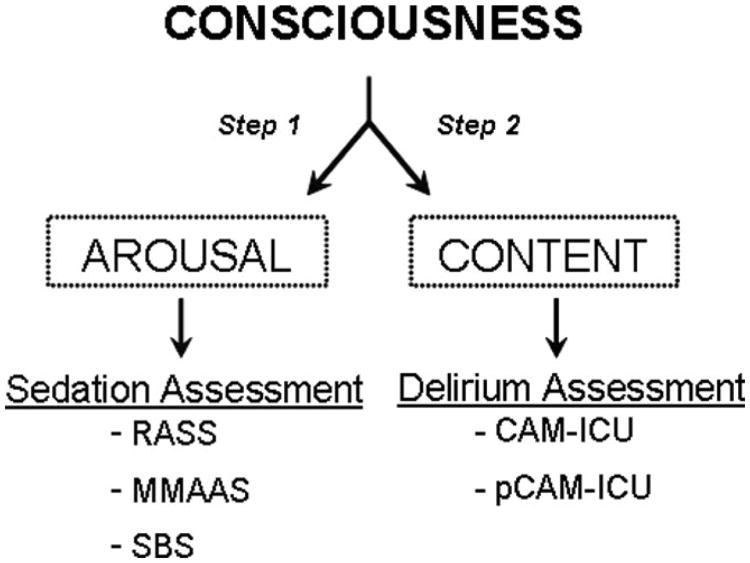
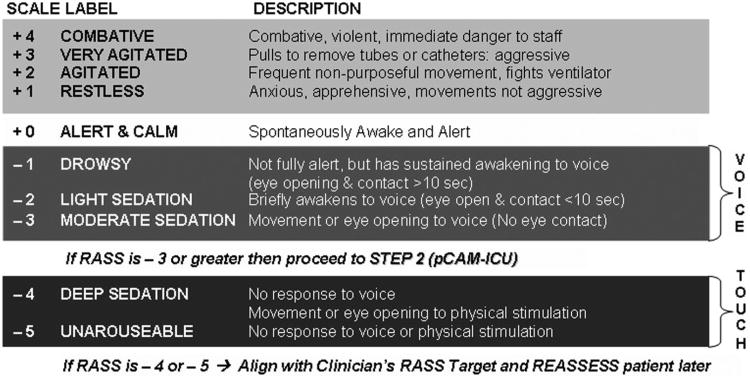
Design and setting: A prospective observational cohort study investigating the Pediatric Confusion Assessment Method for Intensive Care Unit (pCAM-ICU) patients in the pediatric medical, surgical, and cardiac intensive care unit of a university-based medical center.
Patients: A total of 68 pediatric critically ill patients, at least 5 years of age, were enrolled from July 1, 2008, to March 30, 2009.
Interventions: None.
Measurements: Criterion validity including sensitivity and specificity and interrater reliability were determined using daily delirium assessments with the pCAM-ICU by two critical care clinicians compared with delirium diagnosis by pediatric psychiatrists using Diagnostic and Statistical Manual, 4th Edition, Text Revision criteria.
Results: A total of 146 paired assessments were completed among 68 enrolled patients with a mean age of 12.2 yrs. Compared with the reference standard for diagnosing delirium, the pCAM-ICU demonstrated a sensitivity of 83% (95% confidence interval, 66-93%), a specificity of 99% (95% confidence interval, 95-100%), and a high interrater reliability (κ = 0.96; 95% confidence interval, 0.74-1.0).
Conclusions: The pCAM-ICU is a highly valid reliable instrument for the diagnosis of pediatric delirium in critically ill children chronologically and developmentally at least 5 yrs of age. Use of the pCAM-ICU may expedite diagnosis and consultation with neuropsychiatry specialists for treatment of pediatric delirium. In addition, the pCAM-ICU may provide a means for delirium monitoring in future epidemiologic and interventional studies in critically ill children.
Conflict of interest statement
The remaining authors have not disclosed any potential conflicts of interest.
Figures




Comment in
-
On pediatric delirium and the use of the Pediatric Confusion Assessment Method for the Intensive Care Unit.Crit Care Med. 2011 Jan;39(1):220-1. doi: 10.1097/CCM.0b013e318202e635. Crit Care Med. 2011. PMID: 21178548 No abstract available.
-
Diagnosing delirium in critically ill children: Spanish translation and cultural adaptation of the Pediatric Confusion Assessment Method for the Intensive Care Unit.Crit Care Med. 2012 Mar;40(3):1034. doi: 10.1097/CCM.0b013e31823c8b1c. Crit Care Med. 2012. PMID: 22343876 Free PMC article. No abstract available.
References
-
- American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders. Fourth Edition, Text Revision. Washington, DC: American Psychiatric Association; p. 2000.
-
- Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291:1753–1762. - PubMed
-
- Jackson JC, Gordon SM, Hart RP, et al. The association between delirium and cognitive decline: A review of the empirical literature. Neuropsychol Rev. 2004;14:87–98. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
