

A Clinical Trial Comparing Tapering Doses of Buprenorphine with Steady Doses for Chronic Pain and Co-existent Opioid Addiction
- PMID: 20959867
- PMCID: PMC2931595
- DOI: 10.1097/ADM.0b013e3181ba895d
A Clinical Trial Comparing Tapering Doses of Buprenorphine with Steady Doses for Chronic Pain and Co-existent Opioid Addiction
Abstract
Objectives: Effective strategies are needed to manage individuals with chronic non-cancer pain and coexistent opioid addiction. This study compared opioid discontinuation and opioid replacement protocols.
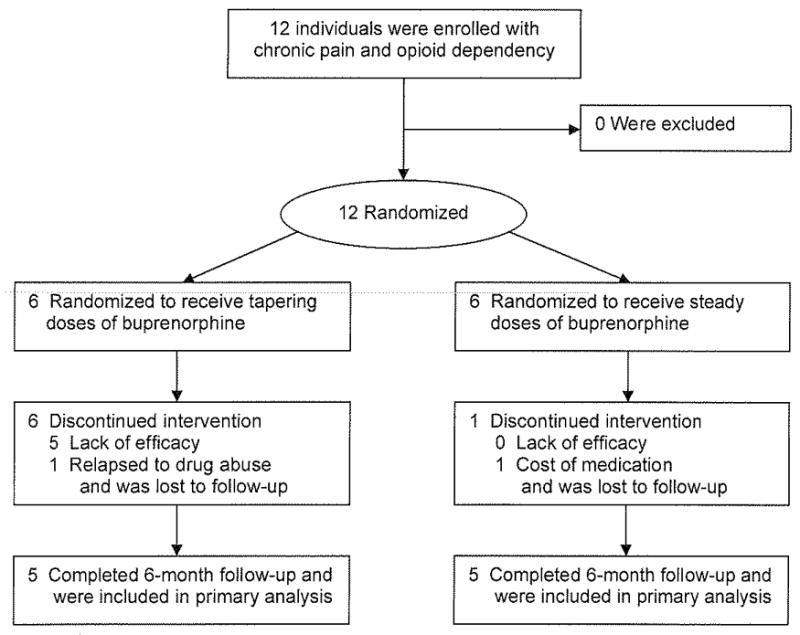
Methods: We planned to enroll 60 individuals into an open-label trial who had been treated with opioids for chronic non-cancer pain, and who also had opioid addiction. Participants were randomly assigned to one of two 6-month treatment protocols of buprenorphine/naloxone sublingual tablets: 1) tapering doses for opioid weaning or "detoxification" (active comparator group) or 2) steady doses for opioid replacement (experimental group). They were followed monthly for the study outcomes: completion of the 6-month treatment protocol and self-reported pain control, physical functioning, alcohol consumption and illicit drug use.
Results: Enrollment was terminated after enrolling 12 participants because none of the 6 assigned to receive tapering doses could successfully complete the protocol (5 were given steady doses and 1 was admitted to an inpatient chemical dependency treatment program); whereas, of the 6 assigned to receive steady doses, 5 completed the protocol (1 withdrew). This difference between the 2 treatment conditions was significant (P = 0.015). Of the 10 participants who completed the 6 month follow-up, 8 reported improved pain control and physical functioning and 5 used alcohol and/or illicit drugs.
Conclusions: We conclude that over 6 months, these participants with chronic pain and co-existent opioid addiction were more likely to adhere to an opioid replacement protocol than an opioid weaning protocol and that opioid replacement therapy with steady doses of buprenorphine/naloxone is associated with improved pain control and physical functioning.
Keywords: Detoxification; addiction; buprenorphine; opioids; pain.
References
-
- Joranson DE, Leitman R. The McNeil National Pain Study. New York: Louis Harris and Associates; 1994.
-
- Turk DC, Okifuji A, Kaluaokalani D. Clinical Outcome and Economic Evaluation of Multidisciplinary Pain Centers. In: Block AR, Kremer EF, Fernandez E, editors. Handbook of Pain Syndromes: Biopsychosocial Perspectives. Mahwah, NJ: Erlbaum; 1999.
-
- Martell BA, O’Connor PG, Kerns RD, et al. Systematic review: opioid treatment for chronic back pain: prevalence, efficacy, and association with addiction. Ann Intern Med. 2007;146:116–127. - PubMed
-
- Manchikanti L, Brown KR, Singh V. National All Schedules Prescription Electronic Reporting Act (NASPER): balancing substance abuse and medical necessity. Pain Physician. 2002;5:294–319. - PubMed
-
- Ballantyne JC, Shin NS. Efficacy of opioids for chronic pain: a review of the evidence. Clin J Pain. 2008;24:469–478. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
