

Multifactorial evaluation and treatment of persons with a high risk of recurrent falling was not cost-effective
- PMID: 20959965
- PMCID: PMC3106152
- DOI: 10.1007/s00198-010-1438-4
Multifactorial evaluation and treatment of persons with a high risk of recurrent falling was not cost-effective
Abstract
Summary: This study evaluated the cost-effectiveness of multifactorial evaluation and treatment of fall risk factors in community-dwelling older persons at high risk of falling. The intervention and usual care groups did not differ in fall risk or costs. The multifactorial approach was not cost-effective compared to usual care in this group.
Introduction: International guidelines recommend multifactorial evaluation and tailored treatment of risk factors to reduce falling in older persons. The cost-effectiveness may be enhanced in high-risk persons. Our study evaluates the cost-effectiveness of multifactorial evaluation and treatment of fall risk factors in community-dwelling older persons at high risk of recurrent falling.
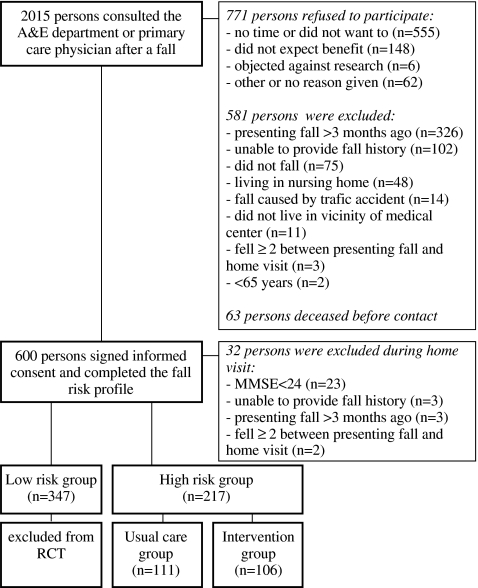
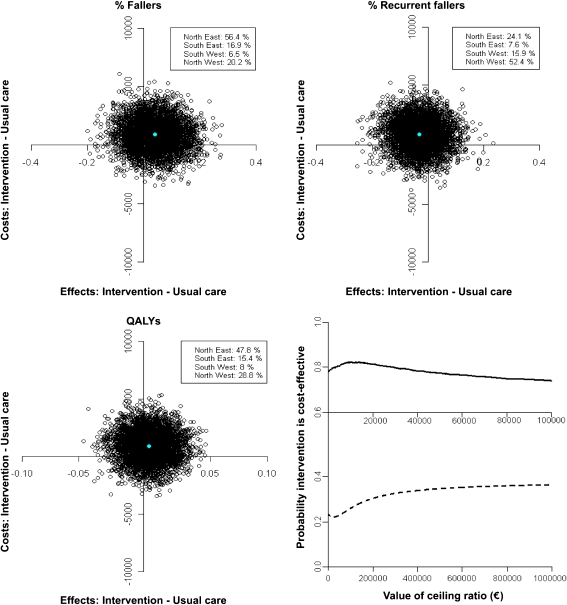
Methods: An economic evaluation was conducted alongside a randomised controlled trial. Participants (≥65 years) with a high risk of recurrent falling were randomised into an intervention (n = 106) and usual care group (n = 111). The intervention consisted of multifactorial assessment and treatment of fall risk factors. Clinical outcomes were proportions of fallers and utility during 1 year. Costs were measured using questionnaires at 3, 6 and 12 months after baseline and valued using cost prices, if available, and guideline prices. Differences in costs and cost-effectiveness were analysed using bootstrapping. Cost-effectiveness planes and acceptability curves were presented.
Results: During 1 year, 52% and 56% of intervention and usual care participants reported at least one fall, respectively. The clinical outcome measures did not differ between the two groups. The mean costs were Euro 7,740 (SD 9,129) in the intervention group and Euro 6,838 (SD 8,623) in the usual care group (mean difference Euro 902, bootstrapped 95% CI: -1,534 to 3,357). Cost-effectiveness planes and acceptability curves indicated that multifactorial evaluation and treatment of fall risk factors was not cost-effective compared with usual care.
Conclusions: Multifactorial evaluation and treatment of persons with a high risk of recurrent falling was not cost-effective compared to usual care.
Figures
References
-
- Murray CJ, Lopez AD. Global and regional descriptive epidemiology of disability: incidence, prevalence, health expectancies and years lived with disability. In: Murray CJ, Lopez AD, editors. The global burden of disease. Boston: Harvard School of Public Health; 1996. pp. 201–246.
-
- Tinetti ME, Doucette J, Claus E, Marottoli R. Risk factors for serious injury during falls by older persons in the community. J Am Geriatr Soc. 1995;43:1214–1221. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
