

Cumulative incidence of cancer among individuals with acquired immunodeficiency syndrome in the United States
- PMID: 20960504
- PMCID: PMC3052856
- DOI: 10.1002/cncr.25547
Cumulative incidence of cancer among individuals with acquired immunodeficiency syndrome in the United States
Abstract
Background: The overall burden of cancer may increase as individuals with acquired immunodeficiency syndrome (AIDS) live longer because of highly active antiretroviral therapy (HAART), which has been widely available since 1996.
Methods: A population-based, record-linkage study identified cancers in 472,378 individuals with AIDS from 1980 to 2006. By using nonparametric competing-risk methods, the cumulative incidence of cancer was estimated across 3 calendar periods (AIDS onset in 1980-1989, 1990-1995, and 1996-2006).
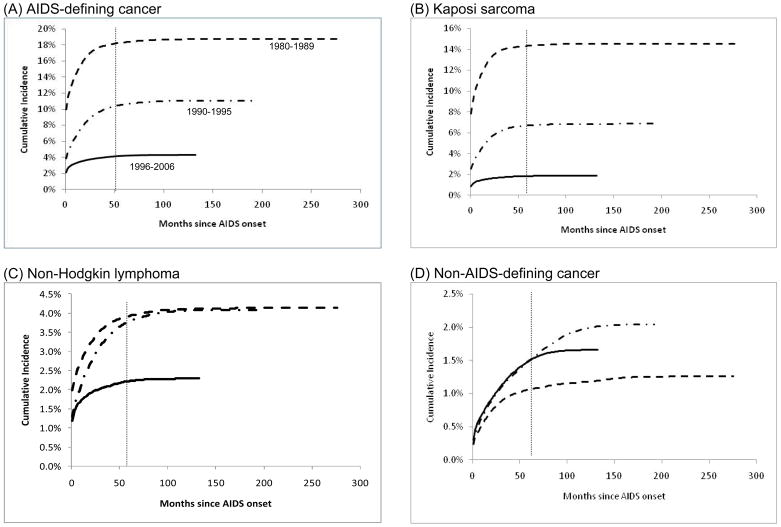
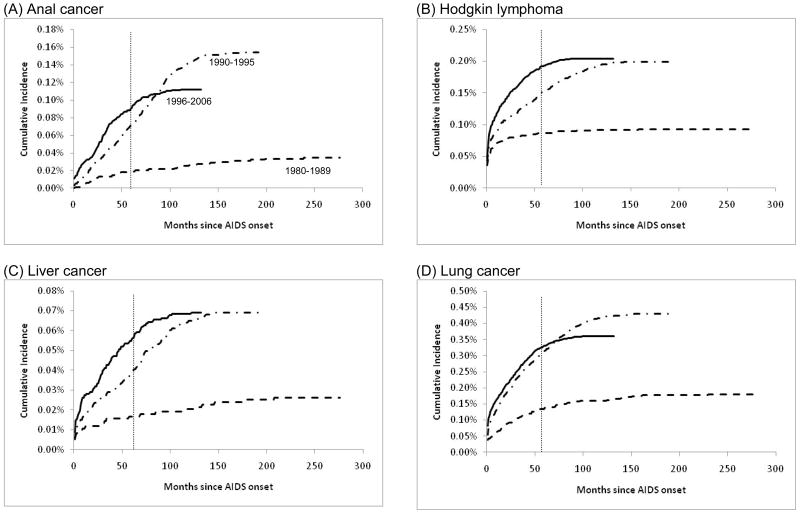
Results: Measured at 5 years after AIDS onset, the cumulative incidence of AIDS-defining cancer (ADC) declined sharply across the 3 AIDS calendar periods (from 18% in 1980-1989, to 11% in 1990-1995, to 4.2% in 1996-2006 [ie, the HAART era]). The cumulative incidence of Kaposi sarcoma declined from 14.3% during 1980 to 1989, to 6.7% during 1990 to 1995, and to 1.8% during 1996 to 2006. The cumulative incidence of non-Hodgkin lymphoma (NHL) declined from 3.8% during 1990 through 1995 to 2.2% during 1996 through 2006; during the HAART era, NHL was the most common ADC (53%). The cumulative incidence of non-AIDS-defining cancer (NADC) increased from 1.1% to 1.5% with no change thereafter (1%; 1996-2006), in part because of declines in competing mortality. However, cumulative incidence increased steadily over time for specific NADCs (anal cancer, Hodgkin lymphoma, and liver cancer). The cumulative incidence of lung cancer increased from 0.14% during 1980 to 1989 to 0.32% during 1990 to 1995, and no change was observed thereafter.
Conclusions: Dramatically declining cumulative incidence was noted in 2 major ADCs (Kaposi sarcoma and NHL), and increases were observed in some NADCs (specifically, cancers of the anus, liver, and lung and Hodgkin lymphoma). As HIV/AIDS is increasingly managed as a chronic disease, greater attention should be focused on cancer screening and prevention.
Published 2010 American Cancer Society.
Conflict of interest statement
Conflicts of interest: All authors declare no conflicts of interest.
Figures
References
-
- Palella FJ, Jr, Delaney KM, Moorman AC, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338:853–60. - PubMed
-
- Palella FJ, Jr, Baker RK, Moorman AC, et al. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV outpatient study. J Acquir Immune Defic Syndr. 2006;43:27–34. - PubMed
-
- Detels R, Munoz A, McFarlane G, et al. Effectiveness of potent antiretroviral therapy on time to AIDS and death in men with known HIV infection duration. Multicenter AIDS Cohort Study Investigators. JAMA. 1998;280:1497–503. - PubMed
-
- Centers for Disease Control and Prevention. 1993 revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. MMWR Recomm Rep. 1992;41:1–19. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
