

Support for anterior temporal involvement in semantic error production in aphasia: new evidence from VLSM
- PMID: 20961612
- PMCID: PMC3037437
- DOI: 10.1016/j.bandl.2010.09.008
Support for anterior temporal involvement in semantic error production in aphasia: new evidence from VLSM
Abstract
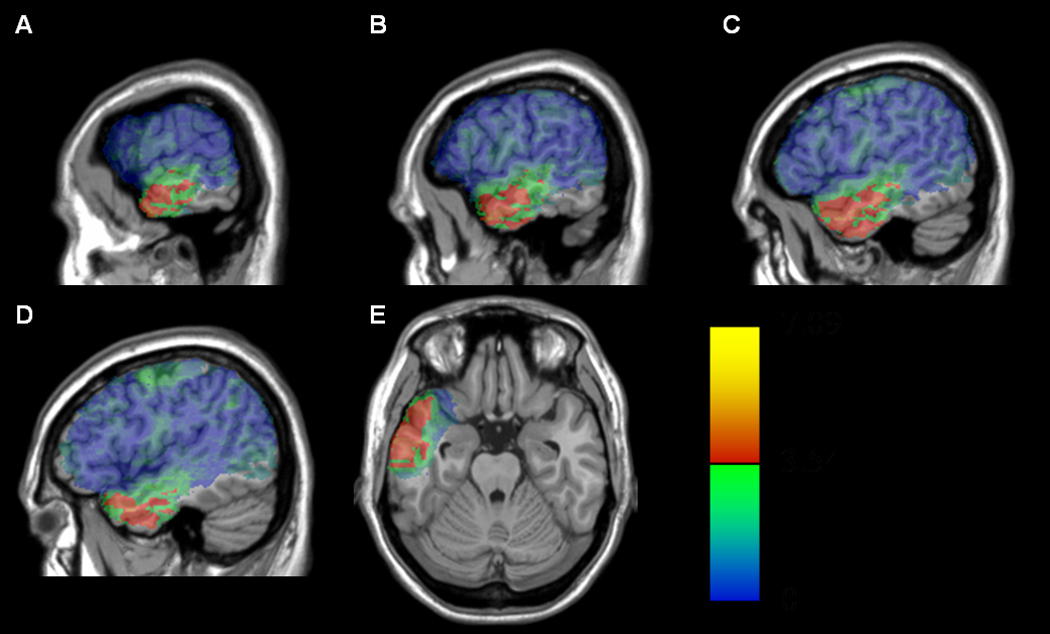
Semantic errors in aphasia (e.g., naming a horse as "dog") frequently arise from faulty mapping of concepts onto lexical items. A recent study by our group used voxel-based lesion-symptom mapping (VLSM) methods with 64 patients with chronic aphasia to identify voxels that carry an association with semantic errors. The strongest associations were found in the left anterior temporal lobe (L-ATL), in the mid- to anterior MTG region. The absence of findings in Wernicke's area was surprising, as were indications that ATL voxels made an essential contribution to the post-semantic stage of lexical access. In this follow-up study, we sought to validate these results by re-defining semantic errors in a manner that was less theory dependent and more consistent with prior lesion studies. As this change also increased the robustness of the dependent variable, it made it possible to perform additional statistical analyses that further refined the interpretation. The results strengthen the evidence for a causal relationship between ATL damage and lexically-based semantic errors in naming and lend confidence to the conclusion that chronic lesions in Wernicke's area are not causally implicated in semantic error production.
Copyright © 2010 Elsevier Inc. All rights reserved.
Figures





References
-
- Avants B, Schoenemann PT, Gee JC. Lagrangian frame diffeomorphic image registration: Morphometric comparison of human and chimpanzee cortex. Medical Image Analysis. 2006;10:397–412. - PubMed
-
- Benson DF, Ardila A. Aphasia: A clinical perspective. New York, NY: Oxford University Press; 1996.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
