

Lipoprotein(a) as a cardiovascular risk factor: current status
- PMID: 20965889
- PMCID: PMC3295201
- DOI: 10.1093/eurheartj/ehq386
Lipoprotein(a) as a cardiovascular risk factor: current status
Abstract
Aims: The aims of the study were, first, to critically evaluate lipoprotein(a) [Lp(a)] as a cardiovascular risk factor and, second, to advise on screening for elevated plasma Lp(a), on desirable levels, and on therapeutic strategies.
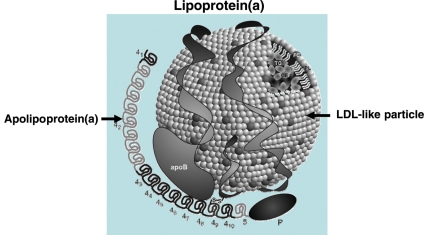
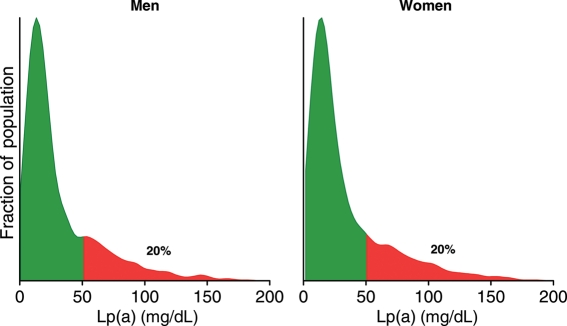
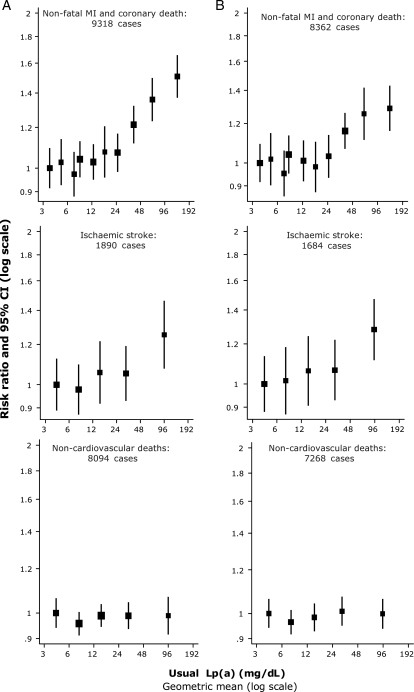
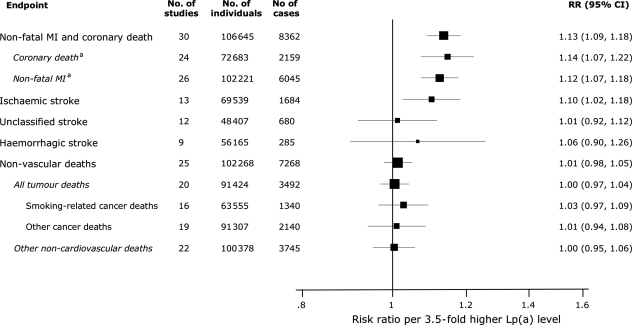
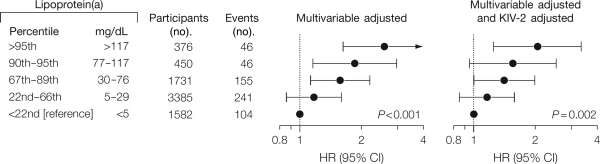
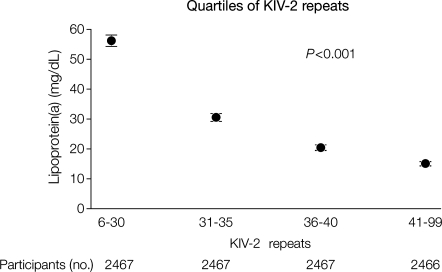
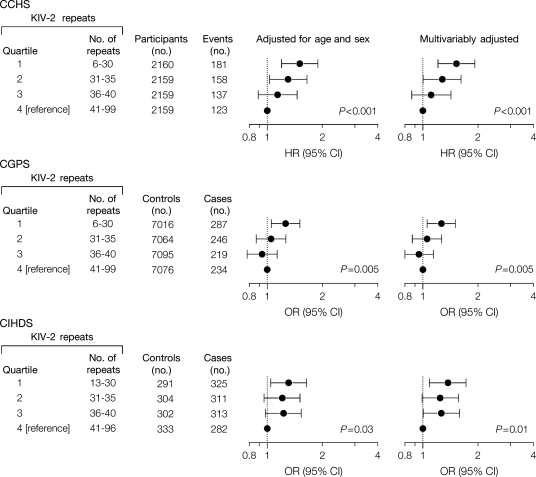
Methods and results: The robust and specific association between elevated Lp(a) levels and increased cardiovascular disease (CVD)/coronary heart disease (CHD) risk, together with recent genetic findings, indicates that elevated Lp(a), like elevated LDL-cholesterol, is causally related to premature CVD/CHD. The association is continuous without a threshold or dependence on LDL- or non-HDL-cholesterol levels. Mechanistically, elevated Lp(a) levels may either induce a prothrombotic/anti-fibrinolytic effect as apolipoprotein(a) resembles both plasminogen and plasmin but has no fibrinolytic activity, or may accelerate atherosclerosis because, like LDL, the Lp(a) particle is cholesterol-rich, or both. We advise that Lp(a) be measured once, using an isoform-insensitive assay, in subjects at intermediate or high CVD/CHD risk with premature CVD, familial hypercholesterolaemia, a family history of premature CVD and/or elevated Lp(a), recurrent CVD despite statin treatment, ≥3% 10-year risk of fatal CVD according to European guidelines, and/or ≥10% 10-year risk of fatal + non-fatal CHD according to US guidelines. As a secondary priority after LDL-cholesterol reduction, we recommend a desirable level for Lp(a) <80th percentile (less than ∼50 mg/dL). Treatment should primarily be niacin 1-3 g/day, as a meta-analysis of randomized, controlled intervention trials demonstrates reduced CVD by niacin treatment. In extreme cases, LDL-apheresis is efficacious in removing Lp(a).
Conclusion: We recommend screening for elevated Lp(a) in those at intermediate or high CVD/CHD risk, a desirable level <50 mg/dL as a function of global cardiovascular risk, and use of niacin for Lp(a) and CVD/CHD risk reduction.
Figures
References
-
- Utermann G. Lipoprotein(a) In: Scriver CR, Beaudet AL, Sly WS, Valle D, editors. The Metabolic and Molecular Bases of Inherited Disease. 8th ed. New York: McGraw-Hill; 2001. pp. 2753–2787.
-
- Kamstrup PR, Tybjaerg-Hansen A, Steffensen R, Nordestgaard BG. Genetically elevated lipoprotein(a) and increased risk of myocardial infarction. JAMA. 2009;301:2331–2339. - PubMed
-
- Clarke R, Peden JF, Hopewell JC, Kyriakou T, Goel A, Heath SC, Parish S, Barlera S, Franzosi MG, Rust S, Bennett D, Silveira A, Malarstig A, Green FR, Lathrop M, Gigante B, Leander K, de FU, Seedorf U, Hamsten A, Collins R, Watkins H, Farrall M. Genetic variants associated with Lp(a) lipoprotein level and coronary disease. N Engl J Med. 2009;361:2518–2528. - PubMed
-
- Matthews KA, Sowers MF, Derby CA, Stein E, Miracle-McMahill H, Crawford SL, Pasternak RC. Ethnic differences in cardiovascular risk factor burden among middle-aged women: Study of Women's Health Across the Nation (SWAN) Am Heart J. 2005;149:1066–1073. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
