

Review
doi: 10.1259/bjr/35714052.
Diagnosis of colonic volvulus: findings on multidetector CT with three-dimensional reconstructions
Affiliations
- PMID: 20965909
- PMCID: PMC3473716
- DOI: 10.1259/bjr/35714052
Item in Clipboard
Review
Diagnosis of colonic volvulus: findings on multidetector CT with three-dimensional reconstructions
Br J Radiol.
2010 Nov.
Abstract
Large bowel volvulus is a rare condition that can occur in patients who present with acute abdominal pain. Radiologists should be able to recognise its appearance on multidetector CT (MDCT) images so that the correct diagnosis can be made and catastrophic consequences can be avoided. In this article, we discuss and illustrate the MDCT and three-dimensional appearance of the various forms of large bowel volvulus. As MDCT allows the precise diagnosis of topography, mechanism and severity, this technique can provide an accurate assessment of large bowel volvulus.
Figures
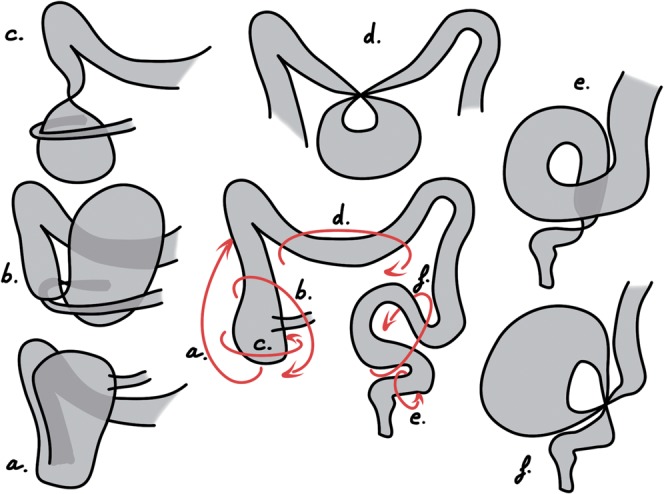
Schematic drawings of the most frequently encountered large bowel volvuli. Each arrow on the diagram of the normal colon represents a possible torsion mechanism, resulting in: a) a bascule type cecal volvulus (CV), b) a loop type CV, c) an axial type CV, d) a transverse colon volvulus, e) an organo-axial sigmoid volvulus and f) a typical sigmoid volvulus.
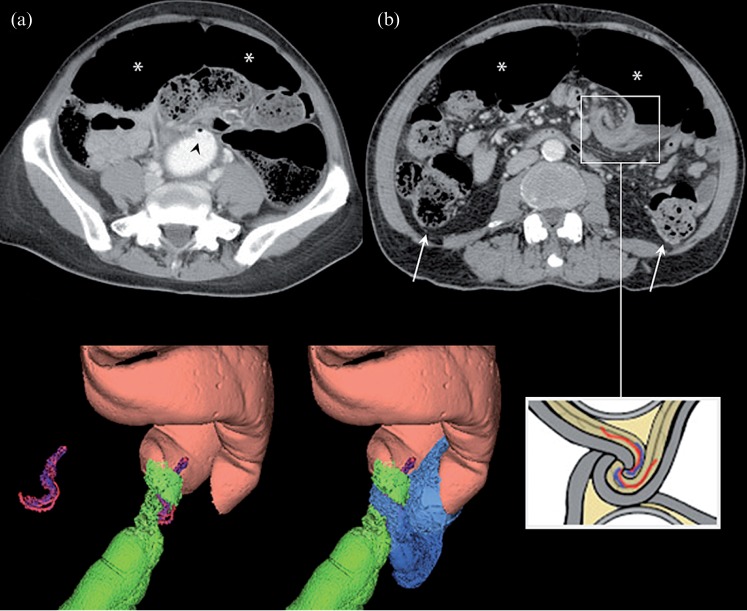
The “whirl sign” and typical appearance of a sigmoid volvulus. (a) Axial CT slice showing a beak sign and no progression of contrast enema beyond the obstruction site (black arrowhead) and the dilated sigmoid loop (*). (b) Axial CT slice centred on the whirl sign of a sigmoid volvulus. Both ends of the dilated loop (*) can be seen, as can the normal upstream colon (white arrows). The three-dimensional reconstructions illustrate the lateral view of a sigmoid volvulus showing the rectum (green), the twisted loop (pink) and the efferent loop (blue). The drawing illustrates the structures involved in the whirl sign.
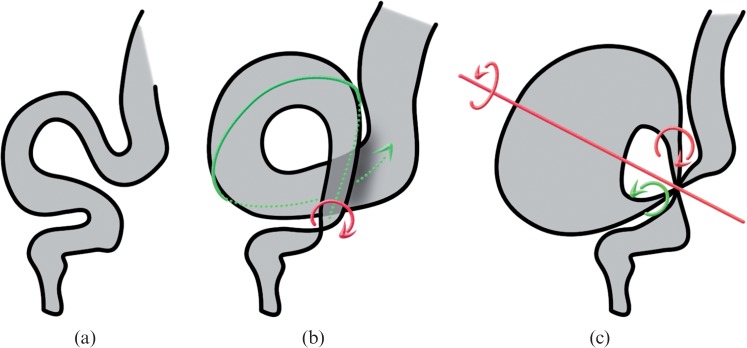
Sketches illustrating the differences between (a) a normal sigmoid colon and a colon with (b) an organo-axial or (c) a mesenterico-axial volvulus. Arrows represent torsion mechanisms, and the resulting mesenterico-axial axis is shown in (c).
A typical sigmoid volvulus (SV) in a 51-year-old woman. (a) Coronal CT slice showing a typical SV and severity signs: dilated loop (*), rectum filled with contrast enema (+) and fully infiltrated mesosigmoid (arrowhead), which can be compared with normal mesentery (double arrowhead). (b) Axial CT slice at the fulcrum point (cranio-caudal axis). Pneumatosis intestinalis of an afferent limb (white arrow), another severity sign, is seen here. The three-dimensional reconstruction shows a closed sigmoid loop (pink) with both limbs of the twisted loop converging toward the fulcrum point, the rectosigmoid junction (green) and the sigmoid-descending colon junction (blue).
An organo-axial sigmoid volvulus in an 86-year-old man. (a) Axial and (b) sagittal CT slices at the fulcrum point show a low-tight whirl sign (cranio-caudal axis) and a beak sign (black arrowhead). In the three-dimensional reconstructions, the sigmoid (pink) follows the twisted rectosigmoid junction (green). The descending colon junction remains out of the twist and the upstream colon is dilated (light blue and semi-transparent).
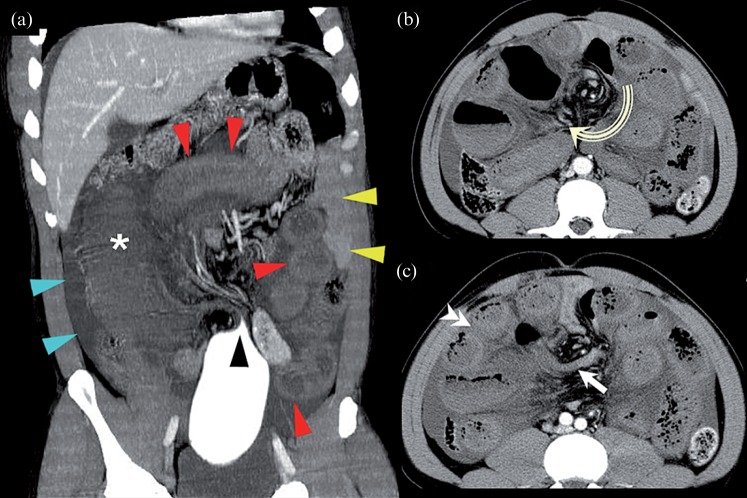
A compound volvulus in a 45-year-old man who presented with signs of shock on admission. (a) Coronal CT slice showing an abrupt stop of contrast enema (black arrowhead), twisted sigmoid (*), twisted ileal loops (red arrowheads), normal small bowel loops in the left flank (yellow arrowheads) and ascites (blue arrowheads). Axial CT slices at the fulcrum point show (b) a large whirl sign (cranio-caudal axis, curved arrow) which includes both limbs of the sigmoid volvulus (arrow) and (c) ileal loops (double arrowhead). Lack of enhancement of the bowel wall after iv injection suggested necrosis.

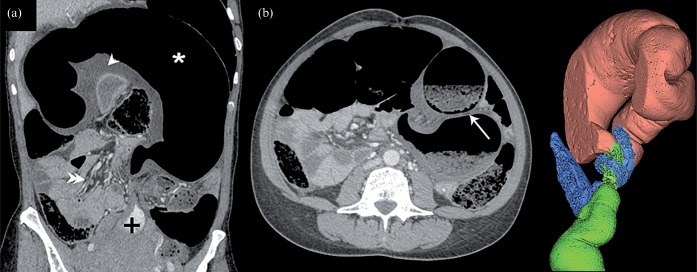
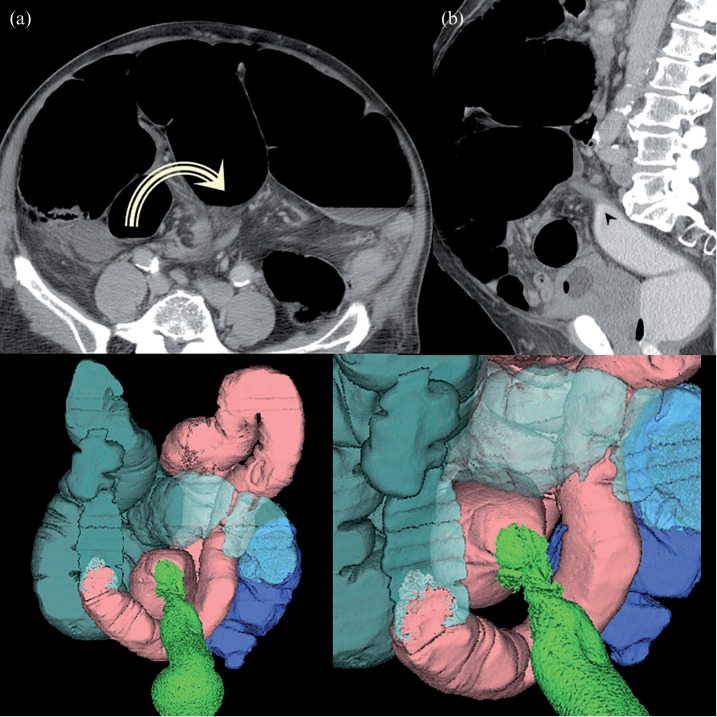
An axial-type volvulus of the caecum in a 56-year-old woman with who presented with signs of shock on admission. (a,b) Coronal CT slices at the fulcrum point demonstrate a tight whirl sign (anteroposterior axis). The caecum remains in the lower part of the abdomen, on the right side. The ileo-caecal region is not involved. There is no free air in the abdominal cavity but severity signs can be seen: there is significant thickening of the caecal wall (white arrowheads) that shows no enhancement and ascites (*) are present. A caecal perforation was present at laparotomy. The three-dimensional (3D) reconstructions show the twist (green) and the colon (pink). The highly distended caecum (blue) has moved up a little, giving the rotation axis an anteroposterior direction. Ileum (purple on top right 3D view) is wrapped around the torsion site but is not included in the whirl sign.

A loop-type volvulus of the caecum in a 74-year-old woman. (a,b) Coronal CT slices from back to front and (c) a sagittal CT slice at the fulcrum point demonstrate a low-tight whirl sign (lateral axis). The caecum (*) is upside down and twisted, and is seen on the left side of the upper part of the abdomen. The three-dimensional reconstructions show the caecum (blue), colon (pink), twist (green) and ileum (red).

Caecal bascule in a 60-year-old man. Even though colonic obstruction is not complete, as suggested by contrast enema reaching the caecum, there is evidence of severity with a highly distended caecum (*) visible on (a) the coronal CT slice and (b) the presence of pneumatosis intestinalis of the caecal wall (white arrow). (b) The sagittal CT slice shows anterior folding of the caecum (lateral axis).
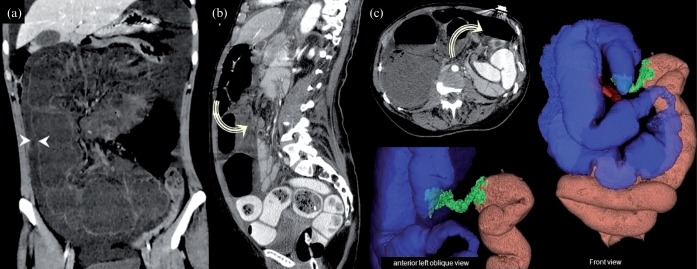
Right hemicolon volvulus in a 59-year-old woman who presented with signs of shock on admission. (a) Coronal, (b) sagittal and (c) axial CT slices at the fulcrum point demonstrate a whirl sign located in the upper and posterior part of the abdomen (lateral axis) and involving the transverse colon. The twisted loop involves the entire right hemicolon (i.e. caecum, ascending colon and half of transverse colon). Severity signs include wall thickening (between arrowheads in (a)) and almost no enhancement of the wall. In the three-dimensional reconstructions, the twist (green) is located in the centre of the transverse colon. The ascending colon and caecum (blue) are in a very unusual position. Thus, the caecum, which can be identified by the terminal ileum (red), is inverted backward.
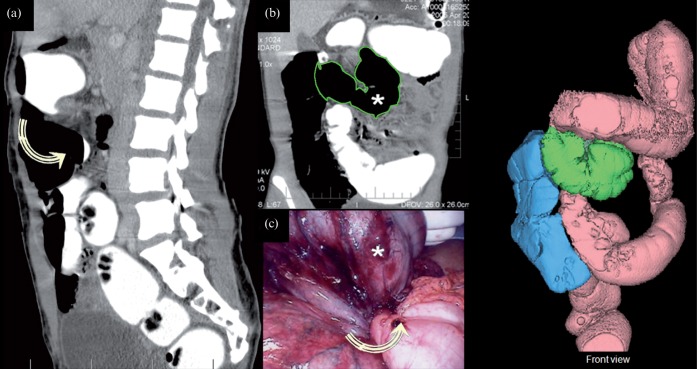
Transverse colon volvulus in a 23-year-old woman. (a) Sagittal and (b) coronal CT slices at the fulcrum point demonstrate a whirl sign that is located in the upper and posterior part of the abdomen (lateral axis). Both limbs of the twisted loop (* with green outline in (b), * in (c)) converge on the transverse colon. The twisted loop involves a segment of the transverse colon. Upstream and downstream colons are seen in the correct position. (c) Peroperative view: free round ligament of the liver creating a strap with no adhesion to the parietal peritoneum. In the three-dimensional reconstructions, the twisted loop (green) is located on the transverse colon. The ascending colon and caecum (blue) are at their usual locations, as are the descending colon and splenic flexure (pink).
References
-
- Ahn SH, Mayo-Smith WW, Murphy BL, Reinert SE, Cronan JJ. Acute nontraumatic abdominal pain in adult patients: abdominal radiography compared with CT evaluation. Radiology 2002;225:159–64 - PubMed
-
- Kellow ZS, MacInnes M, Kurzencwyg D, Rawal S, Jaffer R, Kovacina B, et al. The role of abdominal radiography in the evaluation of the nontrauma emergency patient. Radiology 2008;248:887–93 - PubMed
-
- Madiba TE, Thomson SR. The management of cecal volvulus. Dis Colon Rectum 2002;45:264–7 - PubMed
