

Review
doi: 10.3174/ajnr.A2257.
Epub 2010 Oct 21.
High-resolution MR neurography of diffuse peripheral nerve lesions
Affiliations
- PMID: 20966057
- PMCID: PMC7964353
- DOI: 10.3174/ajnr.A2257
Item in Clipboard
Review
High-resolution MR neurography of diffuse peripheral nerve lesions
AJNR Am J Neuroradiol.
2011 Sep.
Abstract
High-resolution MR imaging of peripheral nerves is becoming more common and practical with the increasing availability of 3T magnets. There are multiple reports of MR imaging of peripheral nerves in compression and entrapment neuropathies. However, there is a relative paucity of literature on MRN appearance of diffuse peripheral nerve lesions. We attempted to highlight the salient imaging features of myriad diffuse peripheral nerve disorders and imaging techniques for MRN. Using clinical and pathologically proved relevant examples, we present the MRN appearance of various types of diffuse peripheral nerve lesions, such as traumatic, inflammatory, infectious, hereditary, radiation-induced, neoplastic, and tumor variants.
Figures
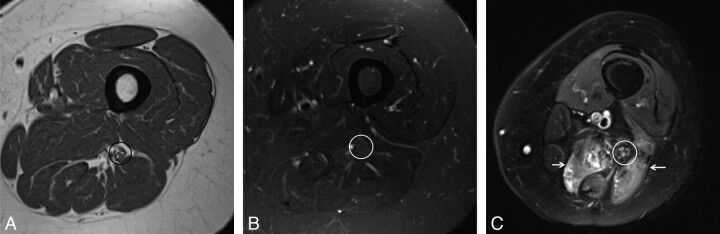
Normal (A and B) versus abnormal (C) MRN appearance of the sciatic nerve. Axial T1WI (A) and T2WI (B) sections at the level of the midthigh show low-intermediate nerve signal intensity (circles). T1WI demonstrates fat planes delineating the normal nerve (perineural fat). C, Axial STIR SPACE at the level of the thighs shows an abnormal sciatic nerve. Notice the enlarged size and T2 hyperintensity of the fascicles. The dark rim of perineural fat is also disrupted. Also note posterior compartment denervation muscle edema (arrows).
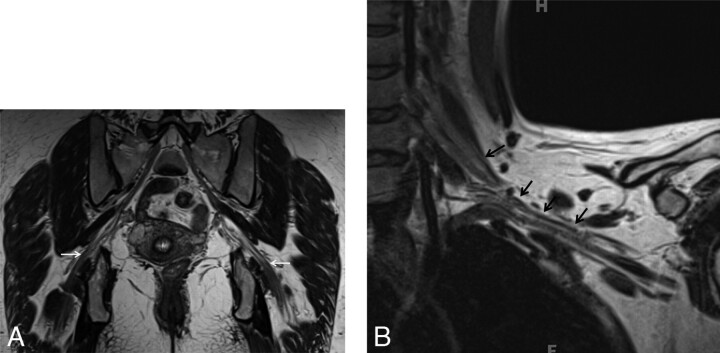
Normal peripheral nerves as seen on SPACE sequences. Coronal 3D T2 SPACE image of the pelvis (A) and coronal 3D T2 SPACE image of the left shoulder (B) depict the normal smooth course of the sciatic nerve and brachial plexus respectively (arrows). Note the smooth course outlined clearly by perineural fat planes.
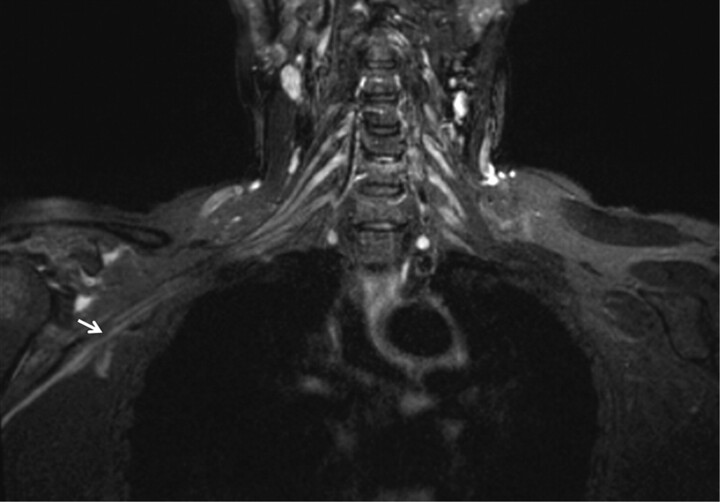
Traumatic neuropathy. A 46-year-old man had a posterior shoulder dislocation during a seizure episode. After the postictal phase, he had weakness of shoulder abduction and sensory loss over the deltoid area. Coronal STIR image shows minimal diffuse nerve enlargement and T2 hyperintensity of the terminal branch of the brachial plexus (arrow) as a result of direct trauma of the recent shoulder dislocation.
Brachial plexus neuritis. A 19-year-old man presented with acute onset of right-shoulder pain without any history of trauma. A week later the pain subsided, but weakness was noted on movement of the right shoulder. On examination, atrophy and severe weakness of abduction of the right shoulder (2/5, Medical Research Council scale for muscle power) were noted. Coronal T2WI shows T2 hyperintense and minimally enlarged right-sided C5 and C6 nerve roots (long arrows) and upper trunks (short arrow), in keeping with acute neuritis. Acute denervation changes were seen in the deltoid and suprascapularis muscles (image not shown).
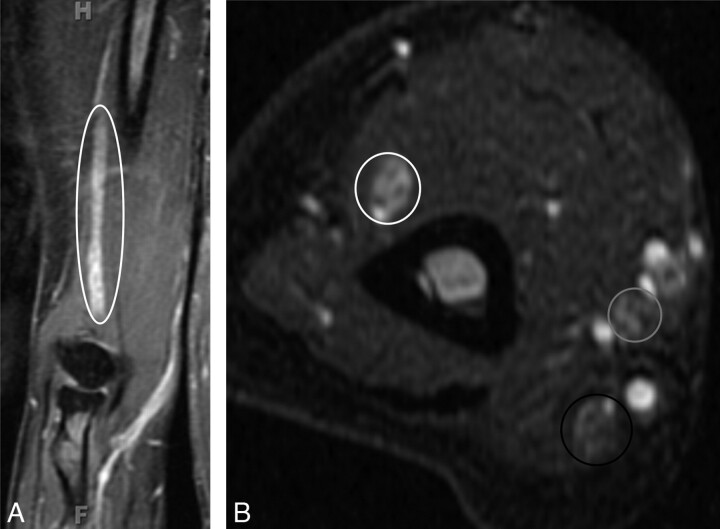
CIDP. A 55-year-old woman presented with a 1-year history of progressive pain in the hands and feet and weakness on finger extension of both hands. On examination, sensory loss and severe weakness in the bilateral distal radial nerve distribution were demonstrated. A nerve-conduction study found severe asymmetric sensory-motor peripheral neuropathy with demyelination (multifocal partial motor conduction block and reduced velocities). A, Coronal contrast-enhanced T1WIFS of the right upper extremity shows an enlarged and enhancing radial nerve (ellipse). The radial, median, and ulnar nerves were enlarged and T2 hyperintense bilaterally with contrast enhancement (images not shown). The diagnosis of CIDP was proved by biopsy in this case. B, Axial STIR image of the right upper extremity shows enlarged and hyperintense radial (white circle), median (gray circle), and ulnar (black circle) nerves. The changes are most pronounced in the radial nerve.
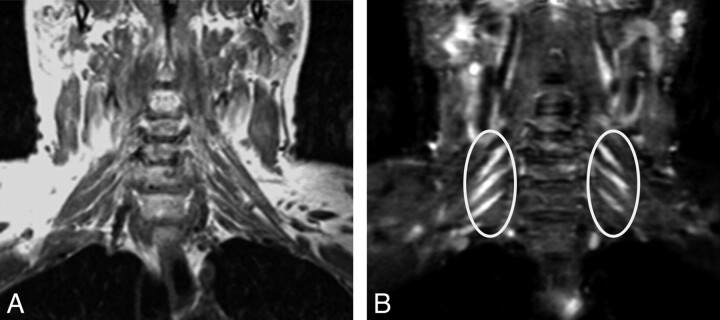
CIDP. A 46-year-old man had an acute episode of pain 2 years before imaging. The pain subsided, but he developed bilateral distal arm paresthesia. Clinical examination at the time of imaging showed distal sensory loss and motor weakness in both arms. Coronal T1 FLAIR (A) and coronal STIR (B) images show T2 hyperintense and symmetrically enlarged brachial plexus nerve roots and trunks (ellipses). The diagnosis of CIDP was proved by biopsy in this case.

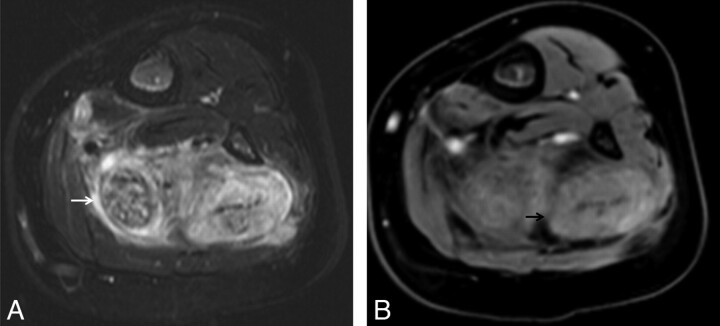
Infectious neuropathy (viral): Hansen disease (leprosy) in peripheral nerves. A 40-year-old man developed multiple small areas of lighter skin on the upper extremity 2 years before imaging. Subsequently, he developed weakness and decreased sensation on the arms and hands. T2WIFS (A) and a proton-attenuation axial (B) image show an enlarged hyperintense median nerve with prominent fascicles continuing into the carpal tunnel (arrows). The diagnosis of leprosy was proved by biopsy.
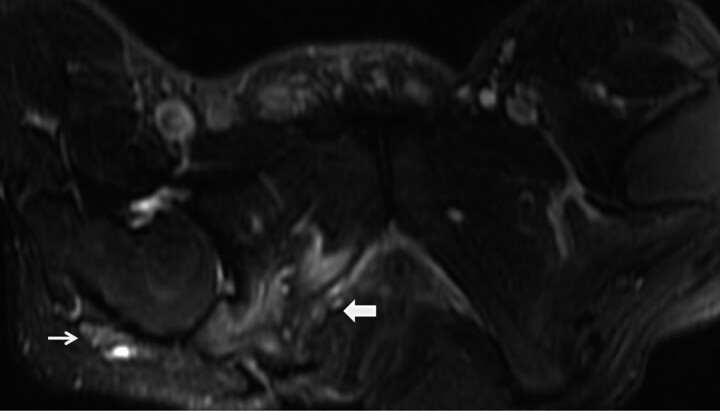
Infectious neuropathy (pyogenic). A 30-year-old man with a history of a long-standing right ischial decubitus ulcer and leg pain developed fever and chills with slow onset of sciatic neuropathy. MR imaging was performed for clinical suspicion of osteomyelitis. Axial T2WIFS shows an abnormally enlarged T2 hyperintense right sciatic nerve (thin arrow). Note the right ischial decubitus ulcer and osteomyelitis (thick arrow). The sciatic nerve demonstrated enhancement on postcontrast images (not shown).

CMT. A 49-year-old man with progressive left hand and arm weakness and numbness, which started approximately 5 years before the current imaging. Coronal T1 FLAIR (A) and coronal STIR (B) images show hyperintense and enlarged brachial plexus nerve roots and trunks with a preserved fascicular pattern (arrows). There is asymmetric involvement of the brachial plexus in this case, with the left side more severely affected than the right side.
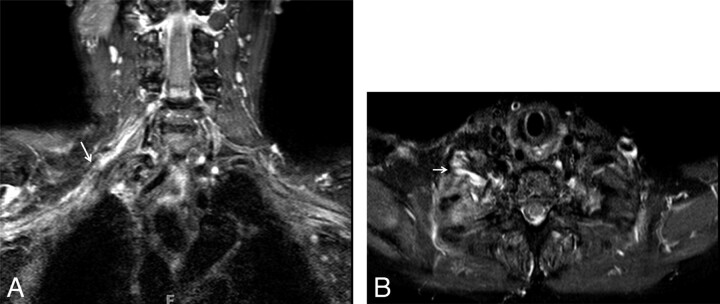
Radiation neuropathy. A 69-year-old woman with a history of breast carcinoma and external beam radiation therapy 2 years before imaging presented with worsening right-arm sensory deficits. Coronal (A) and axial (B) 3D STIR SPACE images show a T2 hyperintense right-sided brachial plexus (arrows) with minimal linear enlargement in the area of the radiation field. No focal mass is visualized.
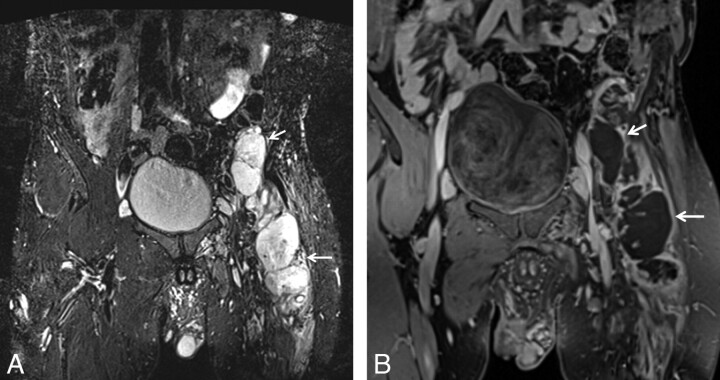
Neurofibromatosis with MPNST. A 57-year-old man with neurofibromatosis presented with persistent left-leg pain and weakness. A, Coronal STIR image shows enlarged lobulated masses (arrows), which represent MPNST in this case. B, Coronal contrast-enhanced T1WIFS shows a heterogeneously enhancing lobulated mass with areas of necrosis along the left femoral nerve, demonstrating MPNST.
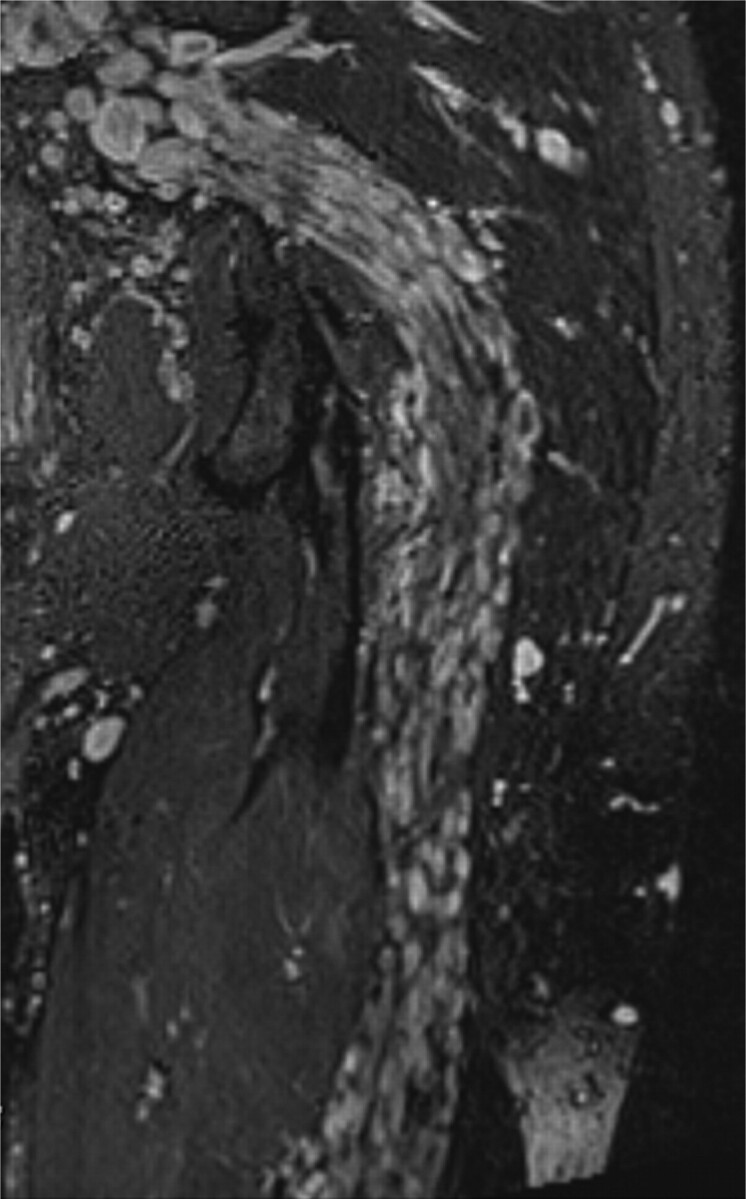
NF1. A 32-year-old man with history of neurofibromatosis underwent MR imaging for bilateral leg weakness. Coronal STIR SPACE image shows a diffusely enlarged left sciatic nerve with innumerable well-circumscribed small masses.
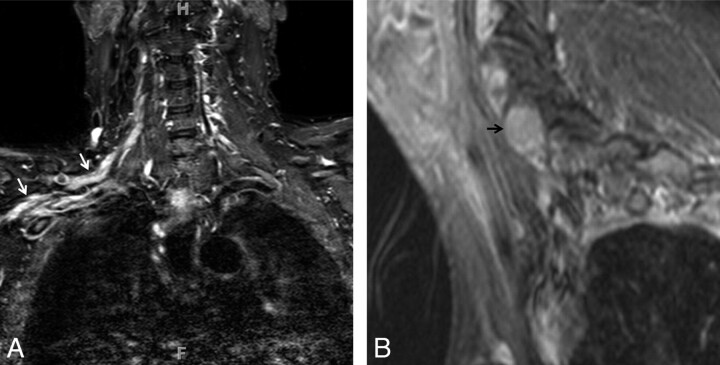
NL: lymphomatous infiltration of the peripheral nerves. A 57-year-old man with B-cell Non-Hodgkin lymphoma presented with right C6 radiculopathy. A, Coronal STIR image shows multifocal segment enlargement of the right-sided brachial plexus (white arrows). B, Sagittal contrast-enhanced T1WIFS shows a focal enhancing mass at the C5–6 neural foramen (arrow). Images obtained after treatment did not show any residual disease (not shown).
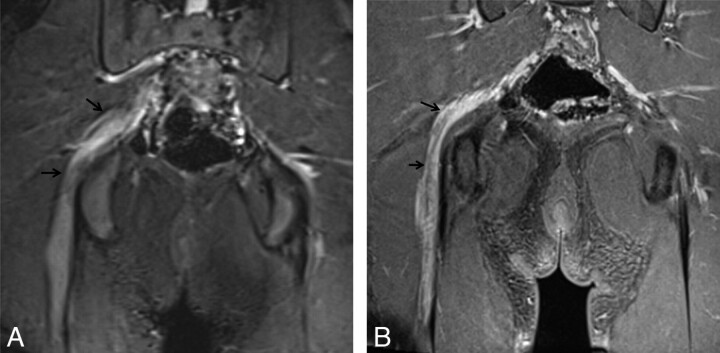
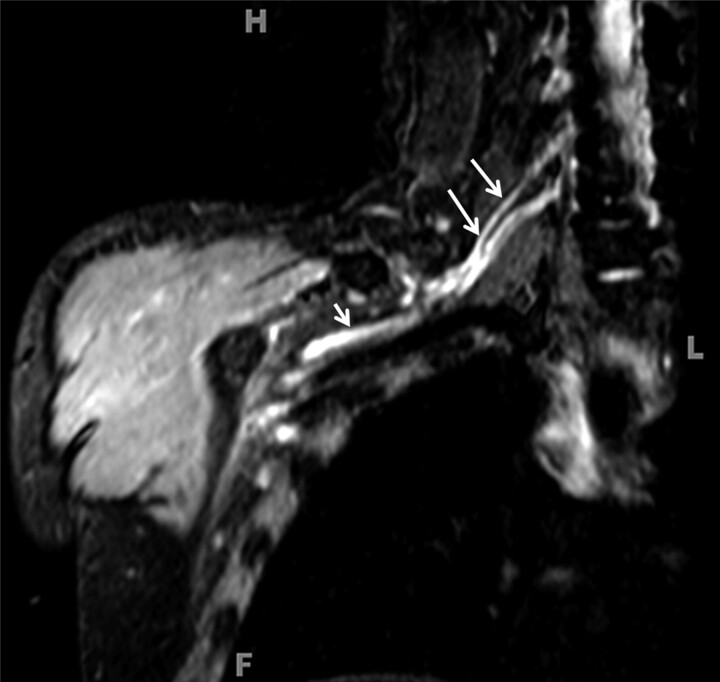
Perineuroma. A 16-year-old boy underwent MR imaging for right sciatic neuropathy with posterior thigh muscle atrophy and weakness. Coronal STIR image (A) and coronal contrast-enhanced (B) T1WIFS show multifocal fusiform enlargement of the right sciatic nerve and enhancement (arrows). Perineuroma was proved by biopsy in this case.
FLH. A 2-year-old boy presented with painless left calf and ankle swelling from 6 months before imaging. Examination of the left lower extremity revealed diffuse swelling throughout the medial aspect of the left calf and ankle. Axial T2WIFS (A) and axial contrast-enhanced T1WI (B) show a fat-containing nonenhancing mass of the tibial nerve with a coaxial cable appearance (arrows).
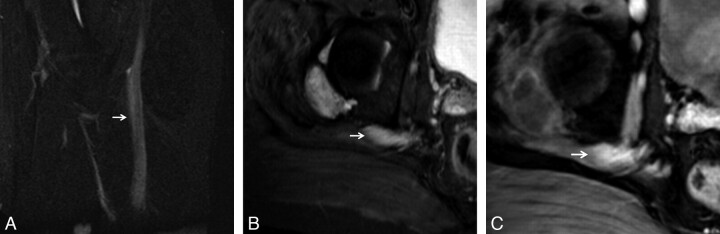
Amyloidosis of the peripheral nerve with amyloidoma. A 24-year-old man presented with a 1-year history of weakness in the right leg before imaging. There were no sensory symptoms. Electromyography and nerve-conduction studies revealed a deficit in the lumbosacral flexor distribution on the right side. A, Sagittal STIR image shows a diffusely enlarged T2 hyperintense right sciatic nerve (arrow). B, Axial STIR image shows localized swelling of the nerve consistent with amyloidoma (arrow). C, Axial contrast-enhanced T1WIFS shows diffuse enhancement in the abnormal sciatic nerve (arrow). Amyloidosis of the nerve was diagnosed by biopsy.
References
-
- Kim S, Choi JY, Huh YM, et al. . Role of magnetic resonance imaging in entrapment and compressive neuropathy: what, where, and how to see the peripheral nerves on the musculoskeletal magnetic resonance image. Part 1. Overview and lower extremity. Eur Radiol 2007;17:139–49 - PubMed
-
- Kim S, Choi JY, Huh YM, et al. . Role of magnetic resonance imaging in entrapment and compressive neuropathy: what, where, and how to see the peripheral nerves on the musculoskeletal magnetic resonance image. Part 2. Upper extremity. Eur Radiol 2007;17:509–22 - PubMed
-
- Amrami KK, Felmlee JP, Spinner RJ.. MRI of peripheral nerves. Neurosurg Clin N Am 2008;19:559–72 vi - PubMed
-
- Kuntz C, 4th, Blake L, Britz G, et al. . Magnetic resonance neurography of peripheral nerve lesions in the lower extremity. Neurosurgery 1996;39:750–56 discussion 756–57 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical