

Oral ondansetron administration in emergency departments to children with gastroenteritis: an economic analysis
- PMID: 20967234
- PMCID: PMC2953527
- DOI: 10.1371/journal.pmed.1000350
Oral ondansetron administration in emergency departments to children with gastroenteritis: an economic analysis
Abstract
Background: The use of antiemetics for children with vomiting is one of the most controversial decisions in the treatment of gastroenteritis in developed countries. Ondansetron, a selective serotonin receptor antagonist, has been found to be effective in improving the success of oral rehydration therapy. However, North American and European clinical practice guidelines continue to recommend against its use, stating that evidence of cost savings would be required to support ondansetron administration. Thus, an economic analysis of the emergency department administration of ondansetron was conducted. The primary objective was to conduct a cost analysis of the routine administration of ondansetron in both the United States and Canada.
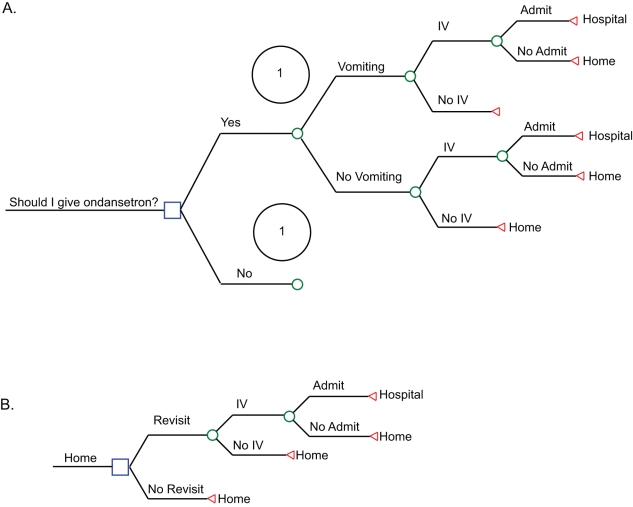
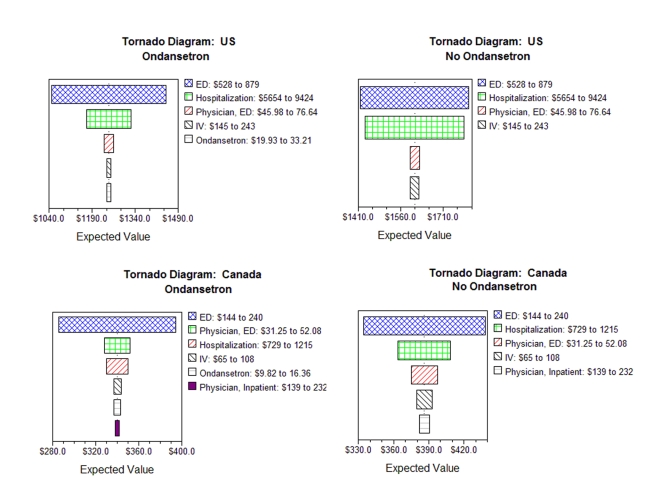
Methods and findings: A cost analysis evaluated oral ondansetron administration to children presenting to emergency departments with vomiting and dehydration secondary to gastroenteritis from a societal and health care payer's perspective in both the US and Canada. A decision tree was developed that incorporated the frequency of vomiting, intravenous insertion, hospitalization, and emergency department revisits. Estimates of the monetary costs associated with ondansetron use, intravenous rehydration, and hospitalization were derived from administrative databases or emergency department use. The economic burden in children administered ondansetron plus oral rehydration therapy was compared to those not administered ondansetron employing deterministic and probabilistic simulations. We estimated the costs or savings to society and health care payers associated with the routine administration of ondansetron. Sensitivity analyses considered variations in costs, treatment effects, and exchange rates. In the US the administration of ondansetron to eligible children would prevent approximately 29,246 intravenous insertions and 7,220 hospitalizations annually. At the current average wholesale price, its routine administration to eligible children would annually save society US$65.6 million (US$49.1-US$81.1) and health care payers US$61.1 million (US$46.2-US$76.3). In Canada the administration of ondansetron to eligible children would prevent 4,065 intravenous insertions and 1,003 hospitalizations annually. Its routine administration would annually save society CDN$1.72 million (CDN$1.15-CDN$1.89) and the health care system CDN$1.18 million (CDN$0.88-CDN$1.41).
Conclusions: In countries where intravenous rehydration is often employed, the emergency department administration of oral ondansetron to children with dehydration and vomiting secondary to gastroenteritis results in significant monetary savings compared to a no-ondansetron policy. Please see later in the article for the Editors' Summary.
Conflict of interest statement
All authors declare that SF, MS, KC have no relationships with GlaxoSmithKline that might have an interest in the submitted work in the previous 3 years; their spouses, partners, or children have no financial relationships that may be relevant to the submitted work; and SF, MS, KC have no nonfinancial interests that may be relevant to the submitted work. SBF does acknowledge that he received research support from GlaxoSmithKline in 2003 but has not had any relationship with them since. He currently receives research support from Institut Rosell Lallemand. KJC previously received research support from GlaxoSmithKline (2000–2004) but has not had any relationship with them since.
Figures
References
-
- Guarino A, Albano F, Ashkenazi S, Gendrel D, Hoekstra JH, et al. European Society for Paediatric Gastroenterology, Hepatology, and Nutrition/European Society for Paediatric Infectious Diseases evidence-based guidelines for the management of acute gastroenteritis in children in Europe: executive summary. J Pediatr Gastroenterol Nutr. 2008;46:619–621. - PubMed
-
- King CK, Glass R, Bresee JS, Duggan C. Managing acute gastroenteritis among children: oral rehydration, maintenance, and nutritional therapy. MMWR Recomm Rep. 2003;52:1–16. - PubMed
-
- Reis EC, Goepp JG, Katz S, Santosham M. Barriers to use of oral rehydration therapy. Pediatrics. 1994;93:708–711. - PubMed
-
- Ozuah PO, Avner JR, Stein RE. Oral rehydration, emergency physicians, and practice parameters: a national survey. Pediatrics. 2002;109:259–261. - PubMed
-
- Li ST, DiGiuseppe DL, Christakis DA. Antiemetic use for acute gastroenteritis in children. Arch Pediatr Adolesc Med. 2003;157:475–479. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
