

Review
doi: 10.1007/s00247-010-1858-5.
Epub 2010 Oct 22.
Hepatobiliary and pancreatic imaging in children-techniques and an overview of non-neoplastic disease entities
Affiliations
- PMID: 20967540
- PMCID: PMC3016234
- DOI: 10.1007/s00247-010-1858-5
Item in Clipboard
Review
Hepatobiliary and pancreatic imaging in children-techniques and an overview of non-neoplastic disease entities
Pediatr Radiol.
2011 Jan.
Abstract
Imaging plays a major role in the diagnostic work-up of children with hepatobiliary or pancreatic diseases. It consists mainly of US, CT and MRI, with US and MRI being the preferred imaging modalities because of the lack of ionizing radiation. In this review the technique of US, CT and MRI in children will be addressed, followed by a comprehensive overview of the imaging characteristics of several hepatobiliary and pancreatic disease entities most common in the paediatric age group.
Figures

Sagittal US image in the midclavicular line shows how to measure the length of the liver in children
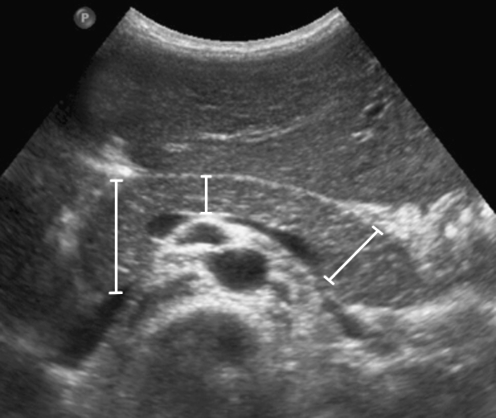
Transverse US image shows the measurements of the head, body and tail of the pancreas in children
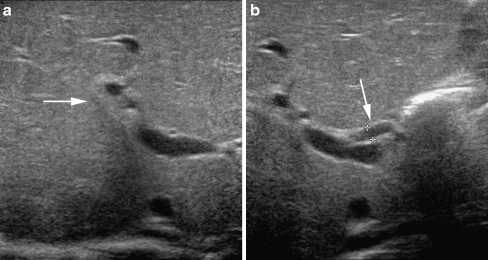
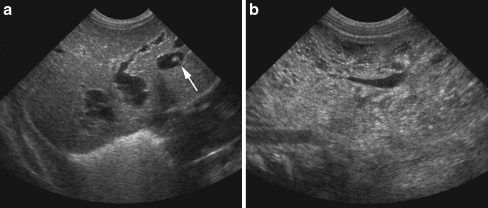
Persistent neonatal cholestasis and biopsy-proven biliary atresia in a 1.5-month-old boy. US shows the triangular cord sign (arrow in a) and increased diameter of the hepatic artery (27 mm, arrow in b)
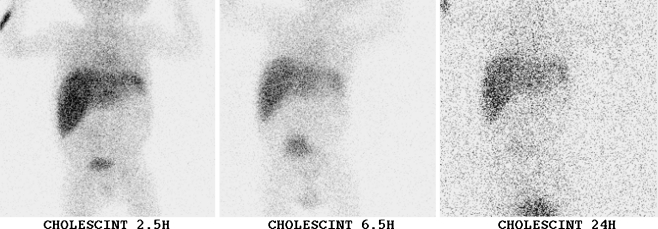
IDA scintigraphy in the same patient as Fig. 3. There is a normal hepatic extraction of the tracer, but no excretion into the GI tract, even on delayed imaging at 24 h after injection of the tracer
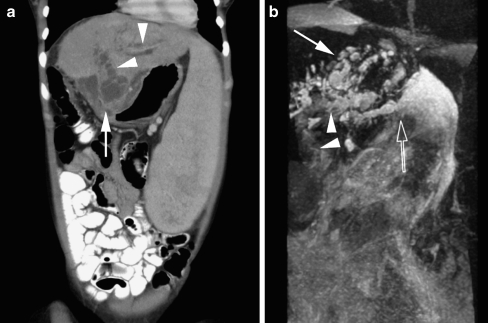
Images in a 19-year-old woman with a history of biliary atresia and Kasai procedure (hepatic portoenterostomy), now presenting with sepsis and cholangitis. a Coronal MPR of the CT scan of the abdomen shows massive splenomegaly, irregular dilatation of the biliary tree (arrowheads) and a complex multiloculated fluid collection (biloma) with the suggestion of a connection with the biliary tree (arrow). b MIP reconstruction of the rt 3-D TSE T2-W sequence also shows the portoenterostomy (arrowheads), irregular dilatation of the biliary tree (closed arrow) and the close relation of the biliary tree to the biloma (open arrow). Furthermore, there is ascites visible surrounding the liver
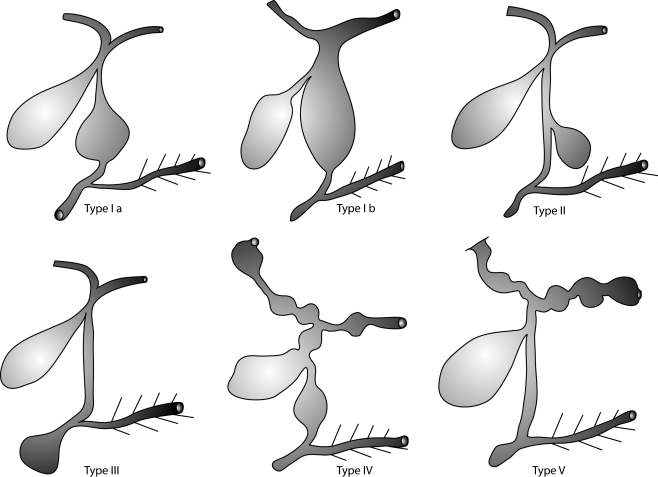
Schematic representation of the classification of choledochal cysts according to Todani: type I, fusiform dilatation of the common bile duct below the cystic bile duct (Ia), or of the common bile duct and main hepatic ducts (Ib); type II, one or more cystic diverticula of the common bile duct; type III, focal dilatation of the distal common bile duct in the papillary region into which the pancreatic ducts drain (also called choledochoceles); type IV, multiple dilatations of the intra- and extrahepatic (IVa) or only the extrahepatic (IVb) bile ducts; and type V, Caroli disease (segmental ectasia of the large intrahepatic ducts throughout the liver)
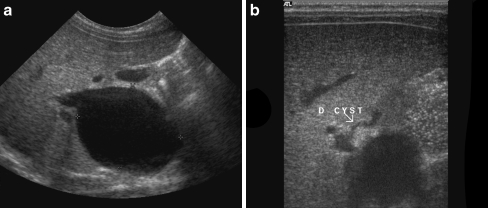
Images in a 2-month-old girl presenting with an antenatally diagnosed (asymptomatic) cyst in the region of the liver. US shows (a) cystic dilatation of the common bile duct, extending from the pancreatic head up to the level where the cystic duct enters the common bile duct. b A type I choledochal cyst
Antenatally diagnosed liver cysts and enlarged kidneys in a 4-day-old boy. a US of the liver shows multiple fusiform and cystic dilatations of the intrahepatic bile ducts. One of the cysts shows the “central dot” sign, representing the portal fibrovascular bundle (arrow); type V choledochal cysts. b US of the kidneys shows enlargement and increased echogenicity with multiple small cysts characteristic of polycystic kidney disease; Caroli disease

MRCP in the same patient as Fig. 7. Oblique coronal thick slab image of a breath-hold 3-D TSE T2-W sequence clearly shows the type I choledochal cyst (arrow)
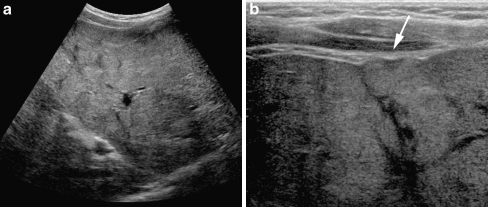
US in a 10-year-old girl with CF. a Transverse US image shows inhomogeneous echogenicity of the liver parenchyma due to liver fibrosis and steatosis. b This detailed transverse US image with a high frequency (12–5 mHz) linear transducer nicely illustrates the undulating contours of the liver parenchyma (arrow) suggesting progression of the liver fibrosis to cirrhosis
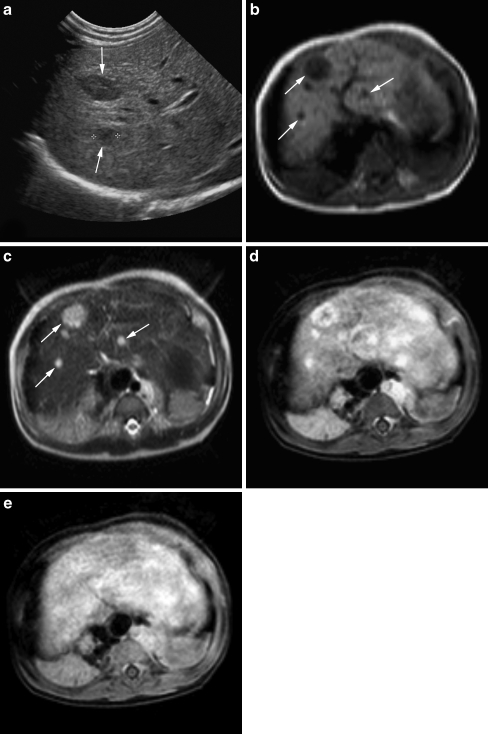
US and MRI in a 6-month-old girl with Beckwith-Wiedemann syndrome. a US shows multiple sharply demarcated hypoechoic lesions throughout the liver parenchyma (arrows). b Axial rt TSE T1-W and (c) rt TSE T2-W images confirm multiple focal liver lesions, dark on T1 and bright on T2. d, e Serial dynamic axial 3-D T1-W images after intravenous contrast administration show early, peripheral nodular or complete enhancement of the lesions and during the late phase, complete fill-in without signs of wash-out. In the clinical setting of Beckwith-Wiedemann the MR signs are compatible with multiple hepatoblastomas or haemangiomas (final histological diagnosis: haemangiomas)

US in a 16-year-old girl with colicky upper abdominal pain. There are multiple echogenic structures with acoustic shadowing visible within the gallbladder compatible with gallstones
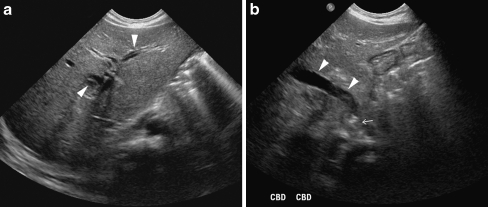
US of the liver in a 2-month-old boy with giant cell hepatitis and cholestasis. US shows intrahepatic biliary dilatation (arrowheads in a), dilatation of the common bile duct (arrowheads in b) and an obstructive echogenic focus in the distal common bile duct at the level of the papilla of Vater (arrow in b), suspicious for an obstructive gallstone

MRCP in a child with cholecysto- and choledocholithiasis. Oblique coronal thick slab image of a bh 3-D TSE T2-W sequence shows multiple filling defects in the gallbladder neck (open arrow) and distal in the common bile duct (closed arrow). Furthermore, there is dilatation of the common bile duct and main hepatic ducts (arrowheads)
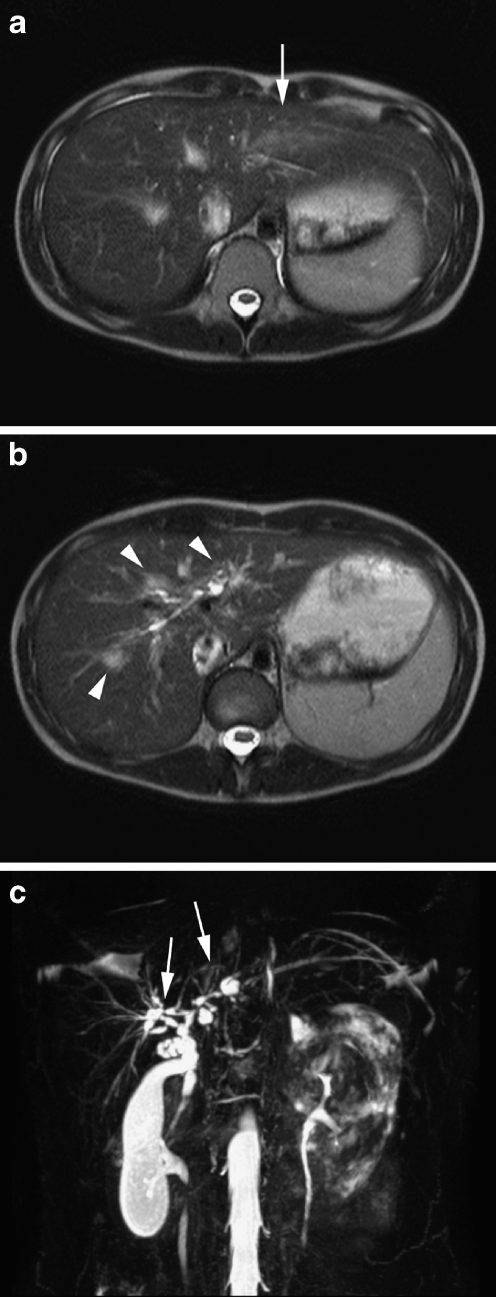
MRI and MRCP in a 10-year-old girl with ulcerative colitis and signs of cholestasis. a, b Axial rt TSE T2-W images show a wedge-shaped area of T2 hyperintensity (arrow in a) as well as periportal parenchymal hyperintensities and biliary duct dilatations (arrowheads in b). c MIP reconstruction of the rt 3-D TSE T2-W sequence clearly illustrates the dilatations and strictures in the common bile duct and central intrahepatic bile ducts (arrows) compatible with primary sclerosing cholangitis
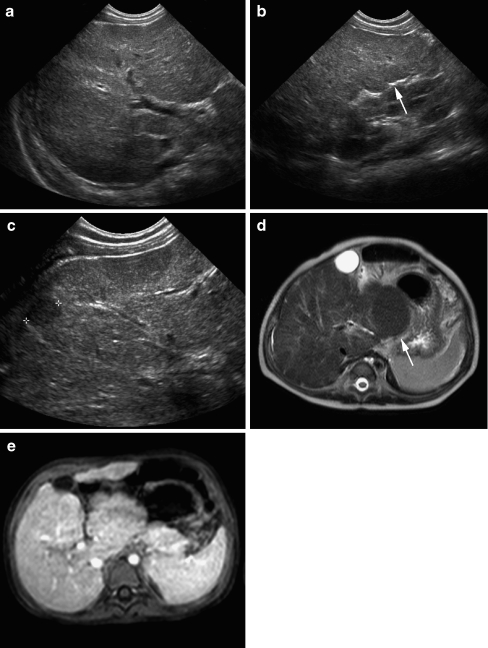
US and MRI in a 10-month-old boy with liver cirrhosis due to a metabolic disease (tyrosinaemia). a–c US shows heterogeneous liver parenchyma with irregular contours (arrow in b) and a small hypoechoic regenerative nodule (c). d rt TSE T2-W image of the liver shows the heterogeneous liver parenchyma with irregular contours and enlargement of the caudate lobe (arrow). e Post-gadolinium bh 3-D GRE T1-W image with fat suppression shows an almost homogeneous enhancement of the liver parenchyma without focal lesions
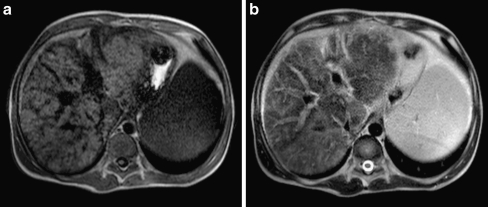
MRI in an 18-year-old boy with a more advanced stage of liver cirrhosis secondary to a mitochondrial disease. a rt TSE T1-W and (b) rt TSE T2-W axial images show marked heterogeneity of the liver parenchyma with multiple low T1signal intensity bands due to fibrotic stranding
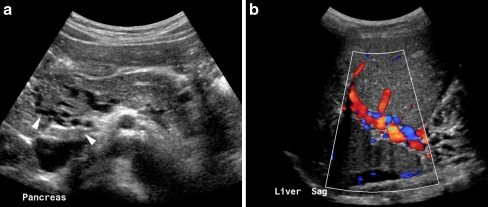
US of the pancreatic head (a) and liver hilum (b) in a 9-year-old boy with a history of portal vein thrombosis. There are multiple collateral vessels visible in the region of the pancreatic head (arrowheads in a) and colour Doppler shows cavernous transformation of the portal vein (b)
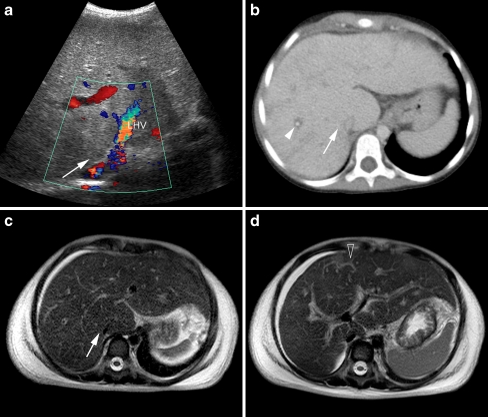
US, CT and MRI in a 8.5-year-old girl presenting with acute abdominal pain and distension. a Colour Doppler US shows heterogeneous hyperechoic liver parenchyma with absent flow in the main hepatic veins of the right hepatic lobe (arrow), LHV left hepatic vein. b Axial CT slice shows slightly heterogeneous enhancement and periportal oedema (arrowhead) as well as absent enhancement of the right hepatic veins (arrow). c and (d) rt TSE T2-W axial MR images show heterogeneous liver parenchyma, ascites, absent right hepatic veins (arrow in c) and intrahepatic collaterals (open arrow in d), compatible with Budd-Chiari syndrome
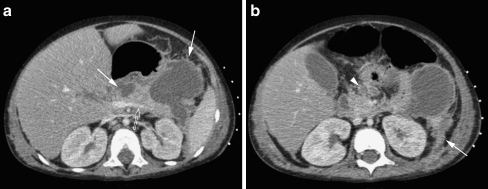
Contrast-enhanced CT in a 3-year-old boy with acute lymphatic leukaemia and acute pancreatitis most likely related to Asparaginase (chemotherapy). The CT shows diffuse gland enlargement with mild inhomogeneous enhancement of the parenchyma (open arrow in a), irregular margins and inflammatory changes of the peripancreatic tissue (arrowhead in b), and multiple small and large peripancreatic fluid collections (arrows in a). The inflammation has spread anteriorly to the pararenal space with thickening of Gerotha’s fascia and peritoneum (arrow in b)
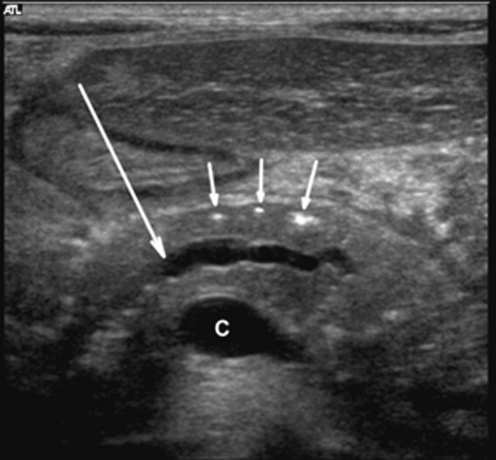
Transverse US image in a 5-year-old boy with chronic hereditary pancreatitis shows the typical features of chronic pancreatitis: calcifications (small arrows) and dilatation of the pancreatic duct (large arrow). C, confluence of the superior mesenteric and splenic veins
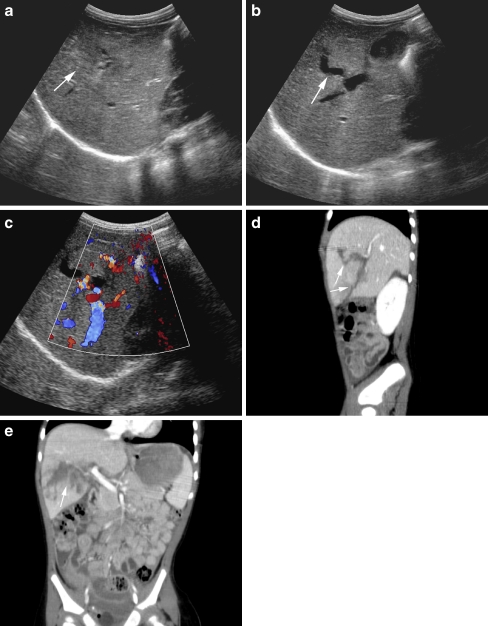
US and CT of the liver in a 1.5-year-old girl with a liver laceration due to blunt abdominal trauma. a–c US shows a heterogeneous defect in the liver parenchyma (arrow in a) with anechoic parts (arrow in b) extending into the liver hilum (c). The sagittal (d) and coronal (e) MPR reconstructions of the contrast-enhanced CT better illustrate the full extent of the liver laceration (arrow in d and e) caudal in the right liver lobe reaching into the liver hilum but without evidence of major vascular injury (grade 4)
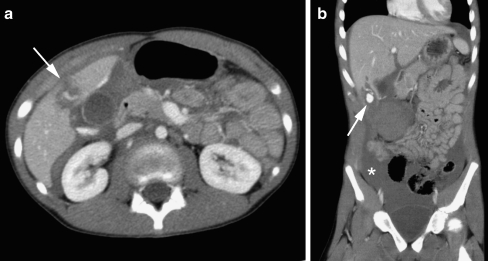
Contrast-enhanced CT of the abdomen in a 12-year-old girl after blunt abdominal trauma. a Axial slice and (b) coronal MPR. There is free intraperitoneal fluid (asterisk in b) and a small liver laceration caudal in the right liver lobe with contrast medium extravasation due to active bleeding (arrow in a and b)
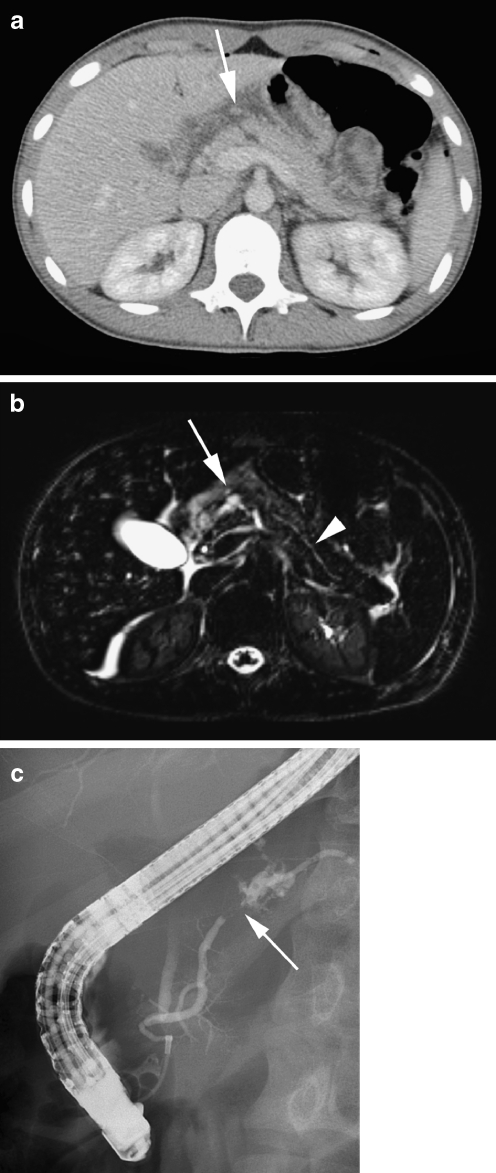
CT, MRI and ERCP in a 14-year-old girl after a bicycle accident (steering-column injury). a Axial contrast-enhanced CT slice and (b) axial T2-W TSE MR image show laceration of the corpus of the pancreas (arrow) with a local retroperitoneal fluid collection, due to haematoma and leakage of pancreatic fluid. The axial MR image shows more clearly the concomitant transection of the pancreatic duct (arrowhead). c ERCP confirms transection of the pancreatic duct (arrow) with extravasation of contrast material (courtesy of R.R. van Rijn, AMC, Amsterdam, The Netherlands)
References
-
- Konus OL, Ozdemir A, Akkaya A, et al. Normal liver, spleen, and kidney dimensions in neonates, infants, and children: evaluation with sonography. AJR. 1998;171:1693–1698. - PubMed
-
- Siegel MJ, Martin KW, Worthington JL. Normal and abnormal pancreas in children: US studies. Radiology. 1987;165:15–18. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
