

The French national prospective cohort of patients co-infected with HIV and HCV (ANRS CO13 HEPAVIH): early findings, 2006-2010
- PMID: 20969743
- PMCID: PMC2988047
- DOI: 10.1186/1471-2334-10-303
The French national prospective cohort of patients co-infected with HIV and HCV (ANRS CO13 HEPAVIH): early findings, 2006-2010
Abstract
Background: In France, it is estimated that 24% of HIV-infected patients are also infected with HCV. Longitudinal studies addressing clinical and public health questions related to HIV-HCV co-infection (HIV-HCV clinical progression and its determinants including genetic dimension, patients' experience with these two diseases and their treatments) are limited. The ANRS CO 13 HEPAVIH cohort was set up to explore these critical questions.To describe the cohort aims and organization, monitoring and data collection procedures, baseline characteristics, as well as follow-up findings to date.
Methods: Inclusion criteria in the cohort were: age > 18 years, HIV-1 infection, chronic hepatitis C virus (HCV) infection or sustained response to HCV treatment. A standardized medical questionnaire collecting socio-demographic, clinical, biological, therapeutic, histological, ultrasound and endoscopic data is administered at enrollment, then every six months for cirrhotic patients or yearly for non-cirrhotic patients. Also, a self-administered questionnaire documenting socio-behavioral data and adherence to HIV and/or HCV treatments is administered at enrollment and yearly thereafter.
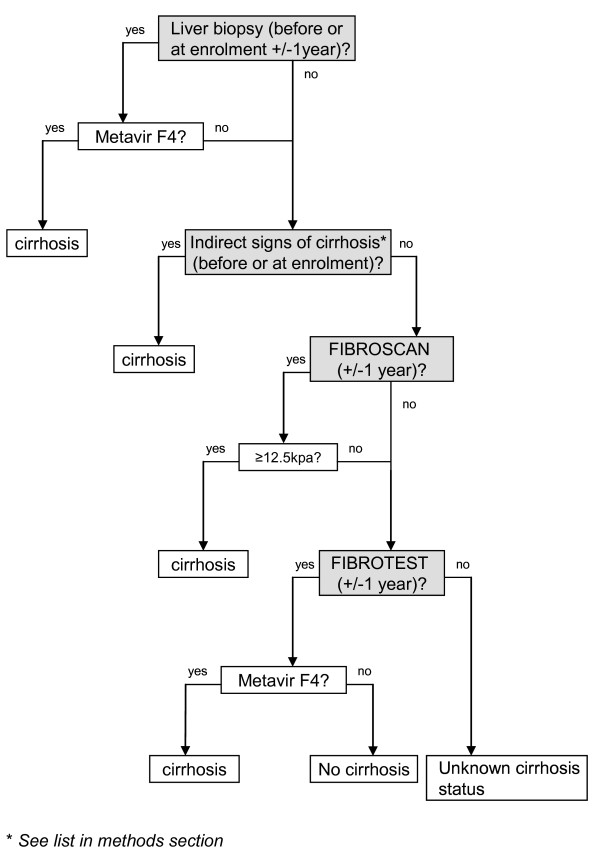
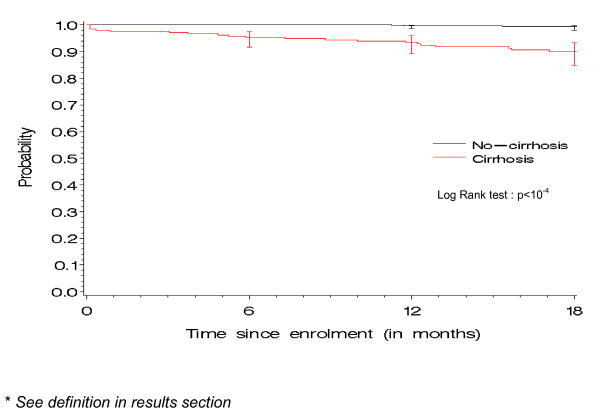
Results: A total of 1,175 patients were included from January 2006 to December 2008. Their median age at enrollment was 45 years and 70.2% were male. The median CD4 cell count was 442 (IQR: 304-633) cells/μl and HIV RNA plasma viral load was undetectable in 68.8%. Most participants (71.6%) were on HAART. Among the 1,048 HIV-HCV chronically co-infected patients, HCV genotype 1 was predominant (56%) and cirrhosis was present in 25%. As of January, 2010, after a median follow-up of 16.7 months (IQR: 11.3-25.3), 13 new cases of decompensated cirrhosis, nine hepatocellular carcinomas and 20 HCV-related deaths were reported, resulting in a cumulative HCV-related severe event rate of 1.9/100 person-years (95% CI: 1.3-2.5). The rate of HCV-related severe events was higher in cirrhotic patients and those with a low CD4 cells count, but did not differ according to sex, age, alcohol consumption, CDC clinical stage or HCV status.
Conclusion: The ANRS CO 13 HEPAVIH is a nation-wide cohort using a large network of HIV treatment, infectious diseases and internal medicine clinics in France, and thus is highly representative of the French population living with these two viruses and in care.
Figures
References
-
- Larsen C, Pialoux G, Salmon D, Antona D, Le Strat Y, Piroth L. et al.Prévalence des coinfections par les virus des hépatites B et C dans la population VIH+, France, juin 2004. Bull Epidemiol Hebd. 2005;23:109–12. [French]
-
- Martin-Carbonero L, Benhamou Y, Puoti M, Berenguer J, Mallolas J, Quereda C. et al.Incidence and predictors of severe liver fibrosis in human immunodeficiency virus-infected patients with chronic hepatitis C: a European collaborative study. Clin Infect Dis. 2004;38:128–33. doi: 10.1086/380130. - DOI - PubMed
-
- Martinez-Sierra C, Arizcorreta A, Diaz F, Roldan R, Martin-Herrera L, Perez-Guzman E. et al.Progression of chronic hepatitis C to liver fibrosis and cirrhosis in patients coinfected with hepatitis C virus and human immunodeficiency virus. Clin Infect Dis. 2003;36:491–8. doi: 10.1086/367643. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
